马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
Laparoscopic Revisional CBD Surgery (Dr. Mariano Palermo).
发布时间:2013-06-16 Clinical Case and Surgical Technique
This is a 29 y/o female that was referred to us after repetitive episodes of ccolic pain.
Her prior surgery was a laparoscopic cholecystectomy for gallbladder stones 14 years after.
Her PMH demonstrates an obese patient with a BMI of 32 . The only previous surgery was a Laparoscopic Cholecystectomy in 1997.
The patients abdomen showed small incisions for the previous surgery.
Her labs were non contributory.
2 ERCPs were performed in 2010 with the impossibility to remove the stones.
In 2011 a new ERCP was performed with unsuccessful results and an endoscopic tenenbaum catheter was used to drain the bile duct.
We can evidence multiple stones, with 2 dominant giant stones. The common hepatic duct was dilated and the distal CBD was normal in size.
So, with a patient with recurrent colic pain 14 years after a laparoscopic cholecystectomy with multiple CBD giant stones and unsuccessful results after 3 ERCPs .... we decided to do a revisional laparoscopic CBD exploration.
After the abdomen was entered under direct vision at the umbilicus using an open technique, a 10-mm trocar was inserted and CO2 was insufflated up to 15 mm of pressure. We used 30° 10-mm laparoscope with 4 more trocars inserted basically in the upper quadrants.
The initial exploration showed multiple adhesions for the previous surgery.
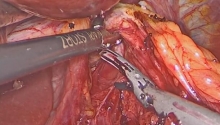
We started to dividing them with scissors trying to expose the CBD.
After free this adhesions from the liver, the CBD was expose.
We the dissect it with scissors and the hepatic artery was seen crossing towards the CBD.
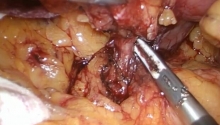
Then, it was separated from the duodenum.
This strong adhesions made some vessels blood.
It can be appreciate the cystic duct and the clips form the previous surgery.
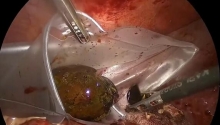
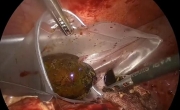
The CBD was opened with scissors ... and we started to remove the stones from the interior of the bile duct.
Intense wash was associated to continue the remotion of the stones. As we can see this giant stones can be removed by this way.
The endoscopic catheter was seen and reinserted in the bile duct.
A T tube was inserted and 2 stichies of multifilament absorbable sutures were used. A cholangiogram was performed and an image compatible with a stone was demonstrated by this method in the right hepatic duct.
The T tube was removed and this stone was taken away by using profuse wash.
The T tube was reinserted and 2 stichies of multifilament sutures were performed.
The first option of treatment in this disease, is an ERCP, papilotomy and the remotion of the stones. Sometimes this treatment is not possible because of giant stones that can not be removed with an ERCP, these is the case of our patient.
Laparoscopic revisional common bile duct exploration is a complex procedure as many revisional surgeries. The difficulties concerns in the multiple adhesions that previous surgeries produce.
After the stichies were done, a drain was placed in the abdomial cavity.
The postOp was unremarkable, with no leaks and the patient was discharged home on postoperative day number 4.
A postoperative cholangiogram was performed with no evidence of CBD stones, good patency and good pass of contrast to the duodenum.
We conclude that laparoscopic revisional CBD exploration for multiple giant stones is a safe and feasible alternative in patients with repetitive colic pain after unsuccessful endoscopic treatment.
|
|

 腹腔镜安全治疗“正中弓状韧带综合征”(MA
腹腔镜安全治疗“正中弓状韧带综合征”(MA
 急性胆囊炎——紧急救治策略
急性胆囊炎——紧急救治策略
 采用腹腔镜经筋膜腹外缝合术修复因 Morgagn
采用腹腔镜经筋膜腹外缝合术修复因 Morgagn
 腹腔镜全胃切除术治疗胃癌中采用线性吻合器
腹腔镜全胃切除术治疗胃癌中采用线性吻合器

 发表于 2013-7-18 09:33:15
发表于 2013-7-18 09:33:15


 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 发表于 2013-7-19 14:55:47
发表于 2013-7-19 14:55:47