马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
Frequently Asked Questions on the Thoracoscopic Decortication SurgeryWhat is Thoracoscopic Decortication Surgery? Thoracoscopic decortication is surgical procedure proven in the management of empyema. Thoracoscopic decortication is really a a minimal access surgical procedure involving the surgical removal with the surface layer, membrane, or fibrous cover of lung. The thoracoscopic decortication is usually performed when the lung is roofed by the thick, inelastic pleural peel restricting lung expansion. Within a non-medical aspect, decortication may be the removing the bark, husk, or outer layer, or peel of visceral pleura of thorax.
The principles of decortication needs to be followed while utilizing thoracoscopic technology. Other areas of fibrinous material must be drained and also the underlying lung free of a restricting pleural peel to match complete re expansion. Success rates are high and chest tube duration, hospital duration of stay, postoperative pain, and recovery are improved over thoracotomy. Mortality rates are low as are recurrent rates and complications. Conversions to open up thoracotomy tend to be more frequent than after other thoracoscopic procedures, however, this is highly recommended a fitness of sound surgical judgment rather than failure of the technique. Thoracoscopic decortication extends the flexibility in the thoracic surgeon in the coping with pleural space infections and could be useful for diagnosis and treatments for the identical with excellent outcomes.
How the diagnosis is done?
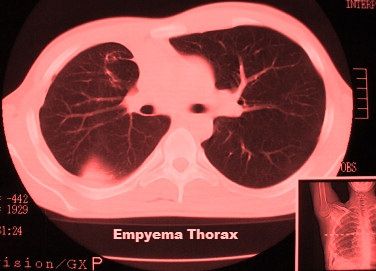
CT scan of the chest provides facts about the positioning, amount of loculation, the extent in the empyema, as well as the underlying lung parenchyma condition. It is not unusual with an organism to not be identified around the pleural fluid culture and thus broad-spectrum antibiotic coverage should be instituted if the carried out empyema is made. This could be modified when the culture data identifies an organism. The appropriate antibiotics are continued to the perioperative period. An evaluation from the patient’s nutritional status should be made and supplemental feedings are initiated if needed. Bronchoscopy must be performed prior to decortication to eliminate endobronchial obstruction within the element of the lung that's trapped from the empyema.
How the thoracoscopic decortication is done?
Thoracoscopic decortication is performed under general anaesthesia. It is a major minimally invasive thoracic operation. Nowadays this procedure can be performed using Video Assisted Thoracoscopic Surgery (VATS). All fibrous tissue is removed from the visceral pleural peel and pus is subsequently drained from the pleural space.
By experienced anaethetist general anesthesia is instituted and lung isolation is accomplished employing a double-lumen endotracheal tube or possibly a single lumen tube with a bronchial blocker. This gives for expansion and collapse of the lung as needed throughout the decortication. Intra-operative monitoring includes an arterial pressure line, large bore intravenous access, a Foley catheter, and pulse oximetry. The individual is put as for a posterolateral thoracotomy.
The digital high definition thoracoscopic camera port is put within the 7th or 6th intercostal space inside the distinctive line of the anterior superior iliac spine. VATS decortication and/or evacuation of hemothorax can be executed through two or three ports. The running port should be placed within the 5th intercostal space relating to the mid and anterior axillary lines. The intercostal incision should allow 3 fingers. A Weitlaner can be used to retract the soft tissues. One third port can be placed posteriorly, positioned allowing accessibility to anterior the main pleural cavity.
When the chest is entered, a suction is utilized to drain the chest area of effusion or blood and as well as a finger accustomed to separation simple loculations. The preoperative CT scan helps guide this ‘blind’ initial drainage and produces a practical pleural space for that thoracoscopic instruments. Gelatinous fibrinous deposits and thrombus are removed with a curved ring forceps clips. The visceral pleural peel can be debrided using ring-forceps, a curette along with a peanut dissector as with a wide open decortication.
Once a pleural space has been given removing fibrinous material is performed on the lateral the main pleural cavity beginning with the apex in the lung and proceeding towards the diaphragm or vice versa. The sucker and ring clamp are utilized together to take out the fibrinous material from your pleural cavity and also the curette, peanut and ring clamp are widely-used to dissect the rind about the lung. On the inferior part of the pleural cavity it is beneficial to identify and separate the low lobe of the lung from your diaphragm. This plane is developed posteriorly and anteriorly allowing for the lung to fill the costodiaphragmatic sulcus when the decortication is done. Next, the posterior part of the pleural space is debrided and the underlying lung is decorticated. Exposure is facilitated by rolling the sufferer anteriorly. Finally, the anterior part of the pleural cavity is debrided along with the lung free of where it really is adherent on the mediastinum. This exposure is improved upon by rolling the individual posteriorly. For the left care have to be taken to protect the phrenic nerve.
By anaesthetist intermittent ventilation with the lung is used to assess the completeness of the decortication since the dissection proceeds. If adequate progress is not being made or there is certainly inadequate expansion of the lung to fill the chest area, then conversion to spread out decortication should be performed. Particular care ought to be taken with hemostasis both about the parietal and visceral pleura
During thoracoscopic decortication surgery once adequate debridement has been accomplished, irrigation is completed and the lung expansion is visualized so that the pleural cavity is filled by the lung. Chest tubes can be put anteriorly and posteriorly for air and fluid drainage. If you find a small space over the diaphragm a right angle tube is positioned with this position to make sure drainage and permit for gradual lung expansion.
After decortication surgery the chest area drain tubes are maintained on suction to be sure there exists complete lung expansion and adequate drainage with the pleural space. After the drainage is below 200cc/day the tubes can be taken off. For patients having an empyema thorax, intravenous appropriate antibiotics are continued throughout the postoperative course and for a further 14 days of oral antibiotics after the patient is discharged. For patients with hemothorax, antibiotics are continued postoperatively for Two days.
Thoracoscopy is additionally indicated in many situation when the nature in the pleural process is undiagnosed, because this enables a directed pleural biopsy which is planning to increase the risk for diagnosis while avoiding the morbidity of the thoracotomy. Other indications for thoracoscopic decortication in some patient include hemothorax and mediastinal debridement in patients with descending mediastinitis.
What are the contraindication of thoracoscopic decortication?
The patient who has gone for prior thoracotomy, prior talc pleurodesis, and previous empyema are generally relative contraindication to thoracoscopic decortication surgery. The inability of some of the terminally ill patient to tolerate single lung ventilation and the presence of a fibrothorax are contraindications to performing thoracoscopic decortication surgery. Patients who develop empyema thorax following esophageal perforation should not be managed thoracoscopically but by thoracotomy.
Consclusion:
Thoracoscopic decortication is proven within the treatments for empyema and the time elapsed considering that the origin from the empyema along with the surgical intervention is probably most predictive in the capability to do the operation successfully. Every area of fibrinous material must be drained along with the underlying lung free of a restricting pleural peel to allow for complete re expansion. Success are high and chest tube duration, hospital period of stay, postoperative pain, and recovery are improved over thoracotomy. Mortality rates are few as are recurrent rates and complications. Conversions to open thoracotomy are sometime required more frequent than after other thoracoscopic procedures, however this should be thought about a fitness of sound surgical judgment as opposed to a failure of the technique. Thoracoscopic decortication extends the versatility from the thoracic surgeon as part of his coping with pleural space infections and could be used for diagnosis and treatment of precisely the same with excellent outcomes.
|
|

 因缺血而行小肠分段切除及一期吻合术
因缺血而行小肠分段切除及一期吻合术
 肌肉活检 _ 如何进行肌肉活检
肌肉活检 _ 如何进行肌肉活检
 尿道下裂修复后包皮瘘和龟头隐裂
尿道下裂修复后包皮瘘和龟头隐裂
 通过外部方法对喉囊肿进行有袋化或去顶
通过外部方法对喉囊肿进行有袋化或去顶

 发表于 2013-2-7 21:26:58
发表于 2013-2-7 21:26:58

 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡










