TISSUE GLUE IN LAPAROSCOPIC INGUINAL HERNIA REPAIR: A RETROSPECTIVE COMPARATIVE ANALYSIS
DR. ABHIJIT MAHANTA
MD (General physician), MS General Surgeon, DMAS
Resident Crimea State Medical University, Ukraine
ABSTRACT:
During the last two decades there have been two revolutions in inguinal hernia repair surgery. First, the introduction of tension-free hernia repair by Liechtenstein in 1989 and then the application of laparoscopic surgery to the treatment of inguinal hernia in the early 1990s. In this context the choice of mesh fixation methods, being an integral part of this procedure remains a topic of arguments and discussions in laparoscopic inguinal hernia repair. There exist many methods of mesh fixation- polyglactin suture, titanium spiral tacks, nitinol anchors, fibrin glue.
Fixation usually uses staples that can lead to nerve injury and chronic post-operative pain. Laparoscopic repairs are associated with a risk of chronic pain of up to 22.5%. The use of fibrin glue may represent an alternative method of mesh fixation preventing the risk of nerve injury.
Keywords: Fibrin sealant, tissue glue, fibrin glue - Tisseel - Inguinal hernia - Laparaoscopic herniorrhaphy - TAPP – TEP, mesh fixation
INTRODUCTION:
Presently the laparoscopic inguinal hernia repair is accomplished by two approaches: transabdominal preperitoneal (TAPP) and totally extraperitoneal (TEP) repair with mesh prosthesis. TAPP is preferred as it manages all types of hernia (direct, oblique, femoral, and obturatory), whether unilateral or bilateral, primary or recurrent. Furthermore, because of its size, the preperitoneal mesh prosthesis covers the entire musculopectineal foramen, where these hernias occur.Among various options available for mesh fixation fibrin glue isbeing used increasingly as an alternative method for hernia surgery, significantly preventing the risk of nerve injury and helping to reduce the incidence of chronic pain. Reliable laparoscopic fixation of meshes prior to their fibrous incorporation minimizes recurrences following transabdominal preperitoneal hernia repair (TAPP) and totally extraperitoneal repair (TEP) repair of inguinal hernias. Various types of staples are available for reliable mesh fixation. However their use has been associated with a certain amount of surgical trauma. Suture-, tack- and staple based fixation systems are associated with postoperative chronic inguinal pain. Reported complications include neuralgia or paresthesia because of nerve entrapments .A chronic form of pubalgia is caused by stapling of the prosthesis to Cooper_s ligament. Bleeding or hematomas in Retzius_ space (muscular, corona mortis) also may occur.
In 1997, Chevrel and Rath first proposed fibrin sealant as an alternate means of mesh fixation in hernia repair, with the aim of reducing the rate of hernia recurrence Canonico later reported the benefits of fibrin sealant in reducing bleeding complications following hernia repair in patients with impaired coagulation. Katkhouda employed a pig model using a total extraperitoneal (TEP) technique to evaluate the tensile strength of mesh fixation 12 days after the use of Tisseel®, demonstrating equal strength to staples. The results of these studies have encouraged surgeons to use fibrin sealant in daily practice as an atraumatic alternative to mechanical mesh fixation .As an atraumatic alternative, the application of fibrin glue (Tissucol/Tisseel, Baxter Healthcare, Deerfield, IL, USA) is a viable and reliable option which keeps mesh in place without the complications associated with stapling. In terms of tensile strength and mesh dislocation, fibrin glue is equivalent to stapling.
AIMS :
The aim of this review article is to evaluate the feasibility and efficacy of use of fibrin glue/tissue glue (tisseel) in laparoscopic inguinal hernia repair, short- and long-term postoperative pain, surgical complications (bleeding, seroma, hematoma, wound infection, incisional hernia, testicular complications). and recurrence rates. This article also emphasizes on evaluation of the advantages and disadvantages of fibrin glue as compared to other methods of mesh fixation, to demonstrate whether fibrin-based mesh adhesion provides adequate biomechanical stability for repair of inguinal hernia by TAPP and TEP and to elucidate the extent to which tacks, anchor based fixations can be replaced with fixation with fibrin glue/ bio adhesives for laparoscopic inguinal hernia repair. The following parameters were also evaluated:
1. Patient selection
2. Operative technique
3. Operating time
4. Intra and post operative complications
5. Post operative pain
6. Hospital stay
7. Cost effectiveness
MATERIALS AND METHODS:
The literature utilized in this article were taken from search engine Google, Springerlink library, Highwire press, Surgical endoscopy journal, World journal of surgery, Medscape. The following terms were used: fibrin glue in laparoscopic hernia repair, TAPP, Fibrin sealant in Hernia repair, role of fibrin glue in TAPP, TEP. 2012 Citations were found. The selected articles were screened for further references.
FIBRIN GLUE:
Fibrin glue/ sealant is a commercial tissue adhesive containing fibrinogen and thrombin. The commercial product is a twocomponent system from human plasma that contains more than fibrinogen and thrombin. The first component contains highly concentrated fibrinogen, Factor XIII, fibronectin, and traces of other plasma proteins. The second component contains thrombin, calcium chloride, and antifibrinolytic agent such as aprotinin. Mixing of the two components leads to activation of fibrinogen and thrombin by calcium chloride and formation and cross-linking of fibrin,leading to the formation of polymerized fibrin chains, duplicating the last step of the coagulation cascade. The fibrinogen component gives tensile strength, thrombin stimulates fibroblast proliferation and aprotinin, an antifibrinolytic agent, enhances the life span of the sealant
|
The required dose of Fibrin Sealant depends on the size of the surface to be covered, as in the following table:Maximum size of the
area to be sealed | Required package sizes of
Fibrin Sealant | 4 cm 2 | 0.5 mL | 8 cm 2 | 1.0 mL | 16 cm 2 | 2.0 mL | 40 cm 2 | 5.0 mL |
|
- Sealer Protein Concentrate (Human), Vapor Heated, freeze-dried
- Fibrinolysis Inhibitor Solution (Bovine)
- Thrombin (Human), Vapor-Heated, freeze-dried
- Calcium Chloride Solution
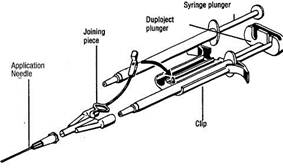
Freeze-dried Sealer Protein Concentrate and Thrombin are reconstituted in Fibrinolysis Inhibitor Solution and Calcium Chloride Solution respectively. The resulting Sealer Protein Solution and Thrombin Solution are then combined (by using the Duploject System, or equivalent delivery device) to form the Fibrin Sealant:
Sealer Protein Concentrate
(Human), Vapor Heated,
Freeze-Dried
| Fibrinolysis Inhibitor Solution
|
| | | solid Fibrin
Sealant | Thrombin (Human),
Vapor Heated, Freeze Dried
| Calcium Chloride Solution
|
| |
Various methods can be used to apply the two components of the sealant , the Duplojet and application needle being the most convenient and popular in laparoscopic surgery.
Commercially Fibrin Sealant is available under the trade name of TISSEEL, marketed by BAXTER and is supplied in four different package sizes of 0.5, 1.0, 2.0 and 5.0 mL, containing the following components:
|
| Package Sizes |
|
| 0.5 mL | 1.0 mL | 2.0 mL | 5.0 mL | Sealer Protein
Concentrate
| Fibrinogen (mg):
| 37.5-57.5 | 75-115 | 150-230 | 375-575 | Total Protein (mg):
| 50-65 | 100-130 | 200-260 | 500-650 | Polysorbate 80 (mg):
| 0.1-0.2 | 0.2-0.4 | 0.4-0.8 | 1-2 | Sodium Chloride (mg):
| 1-2 | 2-4 | 4-8 | 10-20 | Trisodium Citrate (mg):
| 2-4 | 4-8 | 8-16 | 20-40 | Glycine (mg):
| 7.5-17.5 | 15-35 | 30-70 | 75-175 | Fibrinolysis
Inhibitor Solution
| Aprotinin (KIU):
| 1500 | 3000 | 6000 | 15000 | Volume (mL):
| 0.5 | 1.0 | 2.0 | 5.0 | Thrombin
| Thrombin (IU):
| 250 | 500 | 1000 | 2500 | Total Protein (mg):
| 22.5-27.5 | 45-55 | 90-110 | 225-275 | Sodium Chloride (mg):
| 4-6 | 8-12 | 16-24 | 40-60 | Glycine (mg):
| 1.2-1.8 | 2.4-3.6 | 4.8-7.2 | 12-18 | Calcium Chloride
Sodium
| CaCl 2 (µmol):
| 20 | 40 | 80 | 200 | Volume (mL):
| 0.5 | 1.0 | 2.0 | 5.0 | Total Combined
Volume (mL):
| 1.0 | 2.0 | 4.0 | 10.0 |
|
Tisseel Kit 0.5 for 0.5 mL of reconstituted Tisseel solution and 0.5 mL Thrombin solution.
Tisseel Kit 1.0 for 1.0 mL of reconstituted Tisseel solution and 1.0 mL Thrombin solution.
Tisseel Kit 2.0 for 2.0 mL of reconstituted Tisseel solution and 2.0 mL Thrombin solution.
Tisseel Kit 5.0 for 5.0 mL of reconstituted Tisseel solution and 5.0 mL Thrombin solution.
|
Operative technique TAPP with fibrin glue mesh fixation
Patient Positioning
The procedure is performed under general anesthesia.The position of the patient is supine with a slight Trendelenburg tilt (15–20_), legs together and arms alongside the body. The surgeon stands on the opposite side of the hernia, and the assistant stands on the other side of the table. The scrub nurse and instrument table are beside the surgeon. The laparoscopy rack lies at the feet of the patient, in front of the surgical team.
Trocar positioning
Pneumoperitoneum is achieved with a Veress needle inserted at the umbilical site. After an endoabdominal pressure of 12-14 mmHg has been obtained, the first 10-mm trocar replaces the needle at the same site. A 30_ scope is inserted. The other two trocars are inserted by transillumination under internal vision (with care taken to avoid the inferior epigastric vessels) at the level of the transverse umbilical line just lateral to the rectus sheath. The 5- to 12- mm operative trocar is always placed on the righthand\ side for both unilateral and bilateral hernias, and a 5-mm trocar is placed on the opposite side. For bilateral hernias, the two operative trocars are placed about 1 cm below the transverse umbilical line. For a unilateral hernia, the trocar would be positioned 1 cm above the line,at the intersection with the midclavear line to create the classic triangulation of base ball diamond concept aimed at the surgical field with the trocars. The assistant operates the scope from the opposite side of the table. Evaluation of the inguinal regions allows all defects of the fascia transversal is to be detected. The main landmarks are the remnants of the umbilical artery, the ligament of Cooper, the epigastric vessels, and the anteriosuperior iliac spine, all of which also allow definition of the hernia type.
Incision of the peritoneum
If the hernia defect is on the right side, after the iliac spine is located by external pressure, the peritoneum is incised with the scissors at this point, and the incision is continued horizontally and medially. For a left-sided defect, the incision is performed from the lateral aspect of the umbilical artery and extended as far as the left iliac spine. Peritoneal dissection follows the hernia orifice completely at about 0.5 to 1 cm from its upper margin, thus freeing the hernia sac from all visceral and parietal connections. Once the peritoneum is incised, it should be lifted bluntly with the scissors to allow seeping of the carbon dioxide (CO2) to assist in peritoneal detachment. Forceps are used to lift the upper peritoneal margin while scissors are used to complete peritoneal detachment and inferior epigastric vessel dissection.
Parietalization
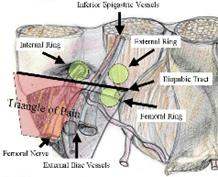
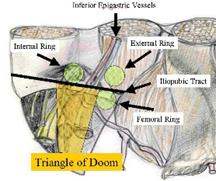
The pressure of the CO2 entering between the peritoneum and the abdominal wall helps dissection and basically requires two instruments: scissors and 5-mm tissue forceps. The inferior peritoneal margin is pulled toward the surgeon with tissue forceps and bluntly dissected from the spermatic cord, which is parietalized to obtain an inverted triangle, with the vas deferens running medially and the genital vessels running laterally between the iliac vessels in the so-called ‘triangle of disaster.’’ Parietalization of the spermatic cord is an important step in the procedure because it allows the freed cord to be placed against the posterior wall. The prosthesis then lodges perfectly on the inguinofemoral wall, thus closing the entire pectineal foramen. Next, the ligament of Cooper is identified by its characteristic consistency and greyish-white color, and dissected. The dissection of Cooper’s ligament is performed bluntly with both instruments, which are divaricated to free the ligament of prevesical fat from the pubic symphysis to the external iliac vein. Once the ligament of Cooper has been prepared, the dissection proceeds toward the upper peritoneal flap, which is bluntly detached using the scissors or traction with two forceps cranially to complete the preparation of the inguinal–femoral wall.
Prosthesis positioning
Once there is sufficient space for placement of the mesh, the next step is the positioning of the prosthesis. Closing of the hernia defect is achieved by means of a nonadsorbable, wide-link mesh that enables the surgeon to recognize the structures on which it is lodged and fixed. To avoid slippage and difficulty in positioning, the mesh should not be too soft. The mesh is introduced by grasping it on the medial and superior margin if the hernia is on the right, and by its superior and lateral margin if the hernia is on the left. Two forceps then spread and position the mesh behind the peritoneal flaps against the posterior wall so as to cover all hernia foramina, Cooper_s ligament, the ‘‘triangle of pain’’, the ‘‘triangle of disaster,’’ the epigastric vessels, and the spermatic cord elements. It is important for the mesh to overlap the hernia foramen by at least 2 cm, and for its medial margin to be alongside the pubic symphysis.
Fixation of the prosthesis
The mesh is fixed with 1 ml of Tissucol for unilateral hernias and 2 ml for bilateral hernias. The prosthesis is fixed along its upper margin, from Cooper_s ligament to the ‘‘triangle of disaster’’ and to the ‘‘tri- angle of pain,’’ using a 3-mm catheter (Duplotip; Baxter Healthcare), which fits the Tisseel syringe. The mesh also may be fixed wherever necessary to increase its stability. Tisseel may be applied in two different ways: by resting the tip of the Duplotip catheter where the mesh is to be fixed and by squeezing out a few drops of glue or the glue seeps across the mesh and fixes it. One also can separate the mesh slightly from the inguinal wall, spray the glue directly on it, and then place the mesh to the wall.
Peritoneal suture
Closure of the peritoneal flap must be performed with extreme care to avoid leaving peritoneal breaches that could allow contact between the mesh and bowel loops.
Mesh prosthesis specifications and design Lateral fixation near the triangle of pain Cooper_s ligament fixation with Tisseel
Operative technique TEP with fibrin glue mesh fixation
The 2 components of the fibrin sealant (Tisseel, Baxter Healthcare Corporation, were reconstituted. Patients is placed in the supine position and general endotracheal anesthesia was induced. A curvilinear incision is made near the umbilicus and carried down to the anterior rectus sheath, which is doubly grasped, elevated, and incised, entering the rectus sheath. The rectus muscles is retracted laterally, exposing the posterior rectus sheath. A peritoneal dissection balloon trocar is inserted and guided by manual and videoscopic guidance down to the level of the pubis where it was inflated and left inflated for several minutes for tamponade effect. It is then deflated, removed and replaced with a structural balloon trocar. Pneumopreperitoneum was instituted under direct vision. Two, 5-mm trocars are placed in the middle hypogastrium, one suprapubically and the second midway between the pubis and the umbilicus. Cooper’s ligament is identified, as well as the cord structures and inferior epigastric vessels. The cord structures is skeletonized, andthe hernia sac is reduced off the internal ring down to the level of the peritoneum. A vertical line is drawn down the long axis of the mesh by using a surgical marker to assist mesh orientation during the procedure. The mesh (8cm x 13cm ) or (10 cm x 15 cm) is placed through the preperitoneum, unfurled, and placed, uncut, over the myopectinate orifice after soaking the mesh in saline for 10 minutes to 15 minutes. The 2 solutions of the fibrin sealant were drawn into separate syringes, which are then fitted into the laparoscopic applicator. Once the mesh is deployed in the position desired, it is secured to the pubic bone (Cooper’s ligament) in the midline, the lacunar ligament, laterally, and superiorly into the transversalis fascia with the fibrin sealant, which is allowed to set for several minutes. The posterior aspect of the matrix repair is then held in place as the pneumopreperitoneum is released under direct vision, observing the peritoneum to obtain its desired position relative to the matrix repair.
In a study by S. Olmi et al (1,10) on fibrin glue mesh fixation in TAPP in 230 patients with 320 hernias (unilateral and bilateral, the results had been encouraging. No perioperative complications were observed. After an average follow-up period of 26 months (range, 1–40 months), the only postoperative complications observed were six seromas (1.8%) and one trocar-site hematoma (0.3%). The mean operating time was 30 min for unilateral hernias and 50 min for bilateral hernias, whether primary or recurrent. Patients usually were discharged the day after surgery and returned to work after 5 days. No patient experienced an inguinal hematoma, which sometimes occurs after stapling. After a mean follow-up period of 26 months (range, 1–40 months), none of the patients reported immediate or late paresthesia or neuralgia. Evaluation of pain levels by the use of a visual analog score indicated that these patients were free of pain by day 7 after surgery. The average operating time was 30 min for unilateral hernias (range, 15–45 min) and 50 min (range, 30–75 min) for bilateral hernias, both primary and recurrent
According to a randomized trial reported by in 93rd Annual Clinical Congress of the American College of Surgeons (ACS), fibrin glue was as effective as staples in preventing hernia recurrence. At the same time, fibrin glue produces less of the postoperative pain experienced with staples, which may cause nerve entrapment. This study enrolled 100 patients scheduled to undergo totally endoscopic pre-peritoneal inguinal hernia repair. Half of the subjects were randomly assigned to fibrin glue and half to staples for mesh fixation. All patients completed the protocol and were available for evaluation for 1 year after the procedure. Pain was reduced with the fibrin glue by several measures. On the first postoperative day, significantly fewer patients in the glue group reported mild pain (28% versus 46% of those receiving staples), and there was a nonsignificant trend toward more glue patients reporting no pain (68% for glue, 42% for staples). One week after the procedure, pain measures still showed a significant advantage for the glue. Using a 10-point visual analogue scale, patients who received glue reported pain in the 0-2 range, while those who received staples reported pain of 3-6. Patients in the glue group also consumed significantly less pain medication (oral diclofenac and paracetamol): a mean of 4.5 tablets per day versus 7.0 tablets per day for the staple group
In a study by Stark et al.(14) the rate of nerve entrapment in laparoscopic patients was 4.2% The genitofemoral nerve was affected with a high frequency (2%), and the ilioinguinal or lateral cutaneous nerve of the thigh was affected in 1.1% of the cases.
The morbidity in post operative period in patients with staples and fibrin glue mesh fixation is a topic of interest. Federico Lovisetto et al (18) carried out an randomized study in 197 patients with inguinal or femoral hernia The primary outcomes were early postoperative and late neuralgia recorded using a visual analog scale (VAS). The effects of neuralgia on functional status were evaluated using the modified SF-36 questionnaire. Secondary outcomes included complications such as nonspecific pain and recurrence. His study included 176 male (89.3%) and 21 female (10.7%) patients with a mean age of 53 years (range, 18–79 years); 188 (95.4%) hernias were inguinal and 9 (4.6%) were femoral. Patient characteristics were similar in the 2 groups. Follow-up visits were done in 1, 3, 6, and 12 months. No intraoperative complications were observed in either of the treatment groups. When compared there was no significant difference in quality of life in the two study groups. The mean duration of intervention was 54 minutes (range, 30–95 minutes) in the Tisseel/fibrin glue group versus 40 minutes (range, 25–105 minutes) in the staples group The mean postoperative hospitalization time in each group was 1 day. The mean recovery time to normal physical activity was 7.9 days (range, 5–11 days) in the fibrin glue group versus 9.1 days (range, 7–11 days) in the staples group. Early postoperative complications which included hematoma/seroma , orchitis, nonspecific pain, occurred in 8% of patients in the fibrin group and in 12% of patients in the staples group.The percentage of Late postoperative complications was 3% and 7% of patients in the fibrin glue and staples groups. There were no cases of hernia recurrences
Over 3 years Graziano Ceccarelli et al (17) compared the characteristics of mesh fixation with titanium clips and fibrin glue (Tisseel) and evaluated if the use of fibrin sealant was as safe and effective as conventional stapling and if there were differences in post-operative pain, complications and recurrences. Comparision was made between two homogeneous groups of 68 patients (83 cases) treated with fibrin glue and 68 patients (87cases) where the mesh was fixed with staples. Transabdominal preperitoneal repair (TAPP) technique was used .Operative times were longer in the group treated with fibrin glue with a mean of 35 minutes (range 22–65 mins) compared to the group treated with staples (25 minutes, range 14–50 mins).The time of hospital stay was the same (24 hours). Postoperative complications, that were more frequent in the stapled group, included trocar site pain, hematomas, intraoperative bleedings and incisional hernias. No significant difference was observed concerning seromas, chronic pain and recurrence rate.
In a study by Arthur P. Fine et al involving 38 adult patients with 51 inguinal hernias. 38 patients with 45 primary and 6 recurrent inguinal hernias were treated with laparoscopic repair by the total extraperitoneal mesh placement (TEP) technique using mesh secured with fibrin sealant. All patients could care for themselves within a day of surgery. Immediately following surgery, patients on average took 7 days off from work. Short-term pain associated with the procedure generally subsided completely within 3 days to 4 days.Follow-up examination 2 weeks after the surgery revealed no swelling or localized abdominal pain, and the patient was allowed full activity and returned to work. Postoperative complications were minor and generally expected as a consequence of surgery (. Mild cord or canal swelling, or both, following the procedure being the most common complaint. The degree of swelling was not judged as severe or necessitating intervention in any case. Mild to moderate orchitis was noted in 3 patients (7.9%) following surgery, as were 2 cases of hematoma (5.3%) and 1 suspected case of seroma (2.6%) that resolved without intervention. Two patients (5.3%) presented with mild fever and localized pain and swelling following surgery. Ciprofloxacin was given for suspected infection, and both patients eventually resolved without further intervention.
P. Topart et al (3) in his retrospective analysis of Tisseel vs tack staples as mesh fixation in totally extraperitoneal laparoscopic repair of groin hernias compared the result of 66 patients with fibrin glue mesh fixation in totally extraperitoneal (TEP) laparoscopic procedure with an earlier series of 102 patients operated on according to the same procedure in which mesh fixation used tack staples. For the fibrin glue group, the operative time was 54 ± 23 min and no difficulty was encountered during preparation or application of the fibrin sealant. There were no reoperations or postoperative deaths. The postoperative course was uneventful for 53 patients (80.3%). Eight patients (12%) had a seroma, which did not require any dedicated treatment in the majority of cases. Three patients (4.5%) had a hematoma: one patient had to remain on calciparin at the time of the operation, and two patients (3%) had a small bowelobstruction. No fever or inflammation were reported after surgery. Overall, patients were discharged 1.5 ± 1.7 days after the operation. In the tack staple group complications occured in 26.4% of the patients. Ten patients (9.8%) had a seroma and eight (7.8%) had a hematoma. No major complications or deaths were reported. The length of stay was a mean of 2.3 days (1.9 days when the additional procedures were excluded). During the follow up three patients (2.9%) developed a recurrence at a mean of 16.3 months after surgery. It was observed that 15 patients (14.7%) complained of pain in the groin area more than 3 months after surgery. There were slightly more seromas but less hematomas in the fibrin glue group compared to the tack staples group, but this was not statistically significant. However, the postoperative chronic pain rate was significantly reduced in the fibrin glue group.
In an animal study in which TEP groin hernia repairs were performed, Katkhouda et al demonstrated (2,4) that graft motion and tensile strength were similar in the staples and fibrin glue groups In addition, histological examinations revealed that the fibrin glue triggered a stronger fibrous reaction and inflammatory response with more fibroblastic mesh ingrowth. The procedures performed laparoscopically in 49 sites. Eighteen grafts were fixed with fibrin glue and 16 with staples; 15 were not fixed. There was no significant difference in graft motion between the fibrin glue and stapled groups, There was no significant difference in median tensile strength between the fibrin glue and stapled groups. fibrin glue triggered a significantly stronger fibrous reaction and inflammatory response than in the stapled and control groups. No infection related to method of fixation was observed in any group. The experiment did not involve serial examinations at later dates because fibroblastic ingrowth has already fixed the mesh in position by postoperative day 12, after which further mesh migration or folding is unlikely. It was found out that in addition to its adhesive property, fibrin glueacts as scaffolding for fibroblastic ingrowth that is enhanced by the chemotactic action of its thrombin component
Hung Lau et al studied in his randomized prospective study a total of 93 patients with 186 inguinal hernias who underwent bilateral TEP were randomized to have mesh fixation by either FS (n = 46) or mechanical stapling (n = 47). The FS group consumed significantly less analgesics compared with that of the staple group There was no significant difference in the postoperative pain score at rest and on coughing from the day of operation to postoperative day 6 between the groups
Stefano Olmi et al (1,10) in his randomized prospective study termed” Quantification of pain in laparoscopic transabdominal preperitoneal (TAPP)” involving 600 patients came to the conclusion that postoperative pain ranged from mild pain between 12 hours and 72 hours with Tisseel and it was higher in other methods of mesh fixation: moderate pain with EMS (Ethicon Endo-Surgery, Inc.) to severe pain with Protak at 48-hour follow-up. Significant differences in length of stay occurred, no recurrence or conversion rates were observed among groups, and morbidity was generally lower with Tisseel. Patients using Tissseel also returned to work sooner than as in other mesh fixing devices.. Prostheses were fixed with Protak (Tyco, Norwalk, Conn), EndoANCHOR (Ethicon Endo-Surgery, Inc., Cincinnati, Ohio), EMS (Ethicon Endo-Surgery, Inc.) and Tisseel (Baxter Healthcare, Milan, Italy).
R. H. Fortelny, R. Schwab et al (15) assessed the quality of life in a trial with mesh fixation with fibrin glue in TAPP. TAPP with fibrin mesh sealing was performed in 11 non-selected consecutive patients. A direct control group (e.g. TAPP with staples) was not considered as favourable change in the quality of life in patients with fibrin glue mesh fixation was the tested hypothesis and not the comparison of techniques. Quality of life and pain were assessed preoperatively and 1 year follow up using the SF36 survey and the visual analogue score (VAS). Post 1 year analysis of recurrences or complications were made. The analysis of the unmodifed SF36 revealed a highly significant improvement. The scale ‘social functioning’ (SOCIAL), which belongs to the mental-health-related scale, had also significantly improved. The VAS significantly reduced after 1 year.
In a observational prospective multicenter study involving 1201 patients performed in France B. Descottes et al (16) assessed Tisseel® fibrin glue for atraumatic mesh fixation in inguinal hernia repair. Out of the , 1,201 patients 526 procedures were performed using open techniques and 675 using laparoscopic repairs. Local complications occurred in 4.7% of patients: 3.0% haematoma, 1.4% seroma, 0.3% recurrence. The mean visual analogue scale (VAS)-rated pain scores were 3.2 pre-operatively, 2.3 immediately after surgery and 1.8 at 1 month. Surgeons rated the product as very easy to use.
DISCUSSIONS:
During the past few years, attention has focused on the pain that may arise after groin hernia surgery. Chronic pain after hernia surgery is a complex and controversial problem that affects not only open but also laparoscopic procedures. Three pain syndromes have been identified: somatic, neuropathic, and visceral pain. Besides nerve damage during dissection, thermal injury due to electrocautery, and inflammatory and/or mechanical reaction to the mesh, stapling of the mesh is the mostfrequent evocated mechanism. According to various literature sources There is a great variation in the rate of postoperative chronic pain, ranging from 0.1% to 0.4% and 22.5% in laparoscopic repairs for which staples are used to attach the mesh. Among the explanations for such a wide discrepancy are the range of pain evaluation methods used, which include clinical examination of the patients, phone calls, and mailed questionnaires and tools to score the severity of the pain.For laparoscopic hernia repair the possibility of nerve injury (pain or parasthesia) caused by entrapment from incorrect placement of staples (above all lateral cutaneus femoral nerve, but ilioinguinal, and genitofemoral are also at risk) and epigastric vessels lesion by clips application may be avoided using fibrin glue either in the TAPP technique or in the TEP It seems that not only entrapment but also postoperative fibrous scar around the staples can lead to nerve injury In conventional TAPP, the prosthesis is anchored using metal clips. This is a critical step that requires the utmost attention to avoid damaging the surrounding nerves and blood vessels. Lesions arising due to such intraoperative damage can lead to complications, including hemorrhage, or painful neuralgia during follow-up.The nerves in the inguinal area that are most frequently involved in postoperative pain following TAPP hernia repair include the genitofemoral, lateral cutaneous femoral, and ilioinguinal and iliohypogastric nerves.Lesions of the lateral cutaneous femoral nerve are the most frequent postoperative neurologic complications associated with laparoscopy. Such lesions are the result of damage or entrapment of the nerve during lateral fixation of the mesh to the deep inguinal ring, with pain in the lateral region of thigh. TAPP hernia repair with Tisseel resulted in a low rate of postoperative pain and rapid resumption of normal activities. Postoperative complications affected only 2.2% of the hernias and were readily treated without the need to extend the hospital stay. Importantly, no recurrences have been observed.. These statistics are in favor of fibrin glue mesh fixation, along with other studies which reports postoperative complication rates of 4.6% for hematomas, 2% for neuralgias, and 0.4% for chronic pain. Reported persistent neuralgia with inguinal pain attributable to stapling vary in the literature from 0.5% to 14%.
To date, the series reporting the lowest postoperative chronic pain rates have not used any means of mesh Tamme et al (19) observed 2.55 and 0% chronic pain problems, respectively, after TEP repair, with a recurrence rate of less than 0.6%. However, the largest of these two series did not specify the length of follow up and the other one was a rather small series (n = 89). Although two randomized studies with a short follow up of nonfixed mesh in laparoscopic repairs (one in TEP and the other in TAPP) did show promising results in terms of recurrence justification for routine nonstapling of the mesh in TEP is not yet substantiated .
Studies points to the fact that mesh stapling does play a key role in generating postoperative pain after laparoscopic hernia repair. Mesh fixation with fibrin glue is preferable as it meets the requirements for both efficiency and security of fixation.
The recurrence rate in the fibrin glue was found to be slightly lower than in the tack staples group but did not differ significantly, and the case of recurrence reported in the fibrin glue group is probably related to an inadequate mesh size in a large direct hernia. Overall, the recurrence rate in the fibrin glue group remains within the range most report approve. Inadequate lateral fixation is a main cause of recurrence after both TAPP (36%) and TEP (22%) . The reason for this is that most of the nerves run laterally where no staples can be applied. Gluing a large mesh on the triangles of disaster and pain is likely to stop the prosthesis from lifting and dislocating, thereby avoiding inferomedial and inferolateral recurrence. It is not known if the enhanced inflammatory response induced by fibrin glue may explain the slightly higher rate of seromas in the fibrin glue mesh fixation. There exists no significant difference in the development of postoperative hematomas, even though the rate is slightly lower in fibrin glue mesh fixation, as compared to the tack staplers but the data available are inconclusive to give the credit to the effect of fibrin glue on local hemostasis. Although no comparison is available between the tack staples group and the fibrin glue group in terms of operation duration, the use of Fibrin glue and its application device did not seem to change the mean operative time, which is comparable to that of other series using tackers. This can be attributed primarily to the peritoneum closure using a running laparoscopic suture and the preparation of fibrin glue and its applicator during the hernia sac dissection. From a mechanical standpoint, fixation of the mesh was equivalent to that obtained with clips but prevented complications related to the application of staples (bleeding and hematomas in Retzius’ space, neuralgia, and chronic pain).
The difference in terms of operating costs between the two fixation techniques/methods does tilts in favour of fibrin glue. Two milliliters of Tisseel is available for 149 USD, whereas the single-use Tacker stapler is 287 USD, 300 euros for Endoanchor (Ethicon Endo-Surgery) and 250 euros for Protak (Tyco, Norwalk, CT, USA). On long term prospective , considerable cost savings can be done if postoperative complications (neuralgias, seromas, and hematomas) are reduced and hospital recovery periods are shortened
CONCLUSIONS:
: The use of fibrin glue has a distinct advantage in laparoscopic treatment of inguinal hernias compared with other conventional methods of mesh fixation. The use of fibrin sealant reduces the risk of post- and intra-operative complications such as bleeding, seroma, chronic pain, has a lower incidence of postoperative neuralgia and provides an early faster return to social life. The recurrence rates are similar, but the operative time is slightly longer if the preparation time of the fibrin sealant is taken into consideration. Otherwise the operative time is shorter in fibrin mesh fixation as compared to staples/tacks. Fibrin glue appears to be an effective and alternative to staples, tacks and anchors for mesh fixation. Mesh fixation with fibrin glue is preferable as it meets the requirements for both efficiency and security of fixation.
References
1.S. Olmi, L. Erba, A. Bertolini, A. Scaini, E. Croce Fibrin glue for mesh fixation in laparoscopic transabdominal preperitoneal (TAPP) hernia repair: indications, technique, and outcomes. Surg Endosc (2006) 20: 1846–1850 DOI: 10.1007/s00464-005-0502-1
2.Katkhouda N. A new technique for laparoscopic hernia repair usingfibrin sealant. Surg Technol Int. 2004;12:120 –126.
3. P. Topart, F. Vandenbroucke, P. Lozac_h Tisseel vs tack staples as mesh fixation in totally extraperitoneal laparoscopic repair of groin hernias: A retrospective analysis. Surg Endosc (2005) 19: 724–727 DOI: 10.1007/s00464-004-8812-2
4. Katkhouda N, Mavor E, Friedlander MH, Mason RJ, Kiyabu M, Grant SW, Achanta K, Kirkman EL, Narayanan K, Essani R Use of fibrin sealant for prosthetic mesh fixation in laparoscopic extraperitoneal inguinal hernia repair. (2001) Ann Surg 233: 18–25
5. Ferzli GS, Frezza EE, Pecoraro AM Jr, Ahern KD. Prospective randomized study of stapled versus unstapled mesh in a laparoscopic preperitoneal inguinal hernia repair. J Am Coll Surg 1999; 188:461–465.
6. B. Novik,1,2 S. Hagedorn,3 U.-B. Mo¨ rk,2 K. Dahlin,2 S. Skullman,3 J. Dalenba¨ ck Surg Endosc (2006) 20: 462–467 DOI: 10.1007/s00464-005-0391-3 Fibrin glue for securing the mesh in laparoscopic totally extraperitoneal inguinal hernia repair A study with a 40-month prospective follow-up period
7. S. C. Schmidt1, J. M. Langrehr. Autologous fibrin sealant (Vivostat®) for mesh fixation in laparoscopic transabdominal preperitoneal hernia repair. Endoscopy 2006; 38(8): 841-844DOI: 10.1055/s-2006-944609
8. S. Schulze,1 V. B. Kristiansen,1 B. Fischer Hansen,2 J. Rosenberg3 Biological tissue adhesive for mesh-application:An experimental study Surg Endosc (2005) 19: 342–344 DOI: 10.1007/s00464-004-9054-z
9. Graziano Ceccarelli Æ Luciano Casciola Æ Massimo Codacci Pisanelli Æ. Comparing fibrin sealant with staples for mesh fixation in laparoscopic transabdominal hernia repair: a case control-study Surg Endosc (2008) 22:668–673 DOI 10.1007/s00464-007-9458-7
10. Stefano Olmi, Alberto Scaini, Luigi Erba, Aimone Bertolini, Enrico Croce. Laparoscopic repair of inguinal hernias using an intraperitoneal onlay mesh technique and a Parietex composite mesh fixed with fibrin glue (Tissucol). Personal technique and preliminary results Surg Endosc (2007) 21: 1961–1964 DOI: 10.1007/s00464-007-9355-0
11. C. Schug-Pass Æ H. Lippert Æ F. Ko¨ckerling Fixation of mesh to the peritoneum using a fibrin glue: investigations with a biomechanical model and an experimental laparoscopic porcine model Surg Endosc (2009) 23:2809–2815 DOI 10.1007/s00464-009-0509-0
12. S. Schulze,V. B. Kristiansen,B. Fischer Hansen, J. Rosenberg. Biological tissue adhesive for mesh-application in pigs: An experimental study Surg Endosc (2005) 19: 342–344 DOI: 10.1007/s00464-004-9054-z
13. R. Schwab Æ O. Schumacher Æ K. Junge Æ M. Binnebo¨sel Æ U. Klinge Æ H. P. Becker Æ V. Schumpelick. Biomechanical analyses of mesh fixation in TAPP and TEP hernia Repair Surg Endosc (2008) 22:731–738DOI 10.1007/s00464-007-9476-5
14. Stark E, Oestreich K, Wendl K, Rumstadt B, Hagmuller E (1999) Nerve irritation after laparoscopic hernia repair. Surg Endosc 13:878–881
15. R. H. Fortelny1, R. Schwab2, K. S. Glaser1, K. U. Puchner3, C. May1, F. König4, H. Redl3 and A. H. Petter-Puchner he assessment of quality of life in a trial on lightweight mesh fixation with fibrin sealant in transabdominal preperitoneal hernia 10.1007/s10029-008-0365-1 499-505
16. B. Descottes1 and M. Bagot d’Arc Fibrin sealant in inguinal hernioplasty: an observational multicentre study in 1,201 patientsHernia. 2009 October; 13(5): 505–510.
17. Graziano Ceccarelli1 ,Luciano Casciola1,Massimo Codacci Pisanelli2,Alberto Bartoli1,Lelio Di zitti1, Alessandro Spaziani1, Alessia Biancafarina1, Massimo Stefanoni1 and Alberto Patriti1 Comparing fibrin sealant with staples for mesh fixation inlaparoscopic transabdominal hernia repair: a case control-study 10.1007/s00464-007-9458-7 668-673.
18. Lovisetto, Federico MD; Longoni, Mauro MD Fibrin Glue Mesh Fixation in Hernia Repair Annals of SurgeryNovember 2007 - Volume 246 - Issue 5 - pp 908-909 doi: 10.1097/SLA.0b013e318158a42.
19. C. Tamme1, H. Scheidbach1, C. Hampe1,C. Schneider1 and F. Köckerling1 Totally extraperitoneal endoscopic inguinal hernia repair (TEP) DOI 10.1007/s00464-002-8905-8 190-195

 因缺血而行小肠分段切除及一期吻合术
因缺血而行小肠分段切除及一期吻合术
 肌肉活检 _ 如何进行肌肉活检
肌肉活检 _ 如何进行肌肉活检
 尿道下裂修复后包皮瘘和龟头隐裂
尿道下裂修复后包皮瘘和龟头隐裂
 通过外部方法对喉囊肿进行有袋化或去顶
通过外部方法对喉囊肿进行有袋化或去顶

 发表于 2013-2-7 20:09:34
发表于 2013-2-7 20:09:34







 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡










