Laparoscopic Management of Intra-abdominal Adhesions
Peritoneal adhesion is a common cause of bowel obstruction, pelvic pain and infertility. Proper technique of adhesiolysis is important and operating surgeons should have clear concept of mechanism of adhesion formation.
Normal fibrinolytic activity prevents fibrinous attachments for 72 to 96 hours after surgery and mesothelial repair occurs within 5 days of trauma. Within these 5 days a single cell layer of new peritoneum covers the injured raw area, replacing fibrinous exudates. However, if fibrinous activity of the peritoneum is suppressed, fibroblast will migrate, proliferate and form fibrous adhesion. Collagen is deposited and neovasular formation starts.
The most important factors which suppress fibrinolytic activity and promote adhesion formation are:
· Port wound just above the target of dissection
· Tissue Ischemia
· Drying of serosal surfaces
· Excessive suturing Omental Patches
· Traction of peritoneum
· Blood clots, stones or dead tissue retained inside
· Prolonged operation
· Visceral injury
· Infection
· Delayed postoperative mobilization of patient
· Postoperative pain due to inadequate analgesia.
Contraindications· Hemodynamic instability
· Uncorrected coagulopathy
· Severe cardiopulmonary disease
· Abdominal wall infection
· Multiple previous upper abdominal procedures
· Late pregnancy
Patient Position
The anaesthetized patient is placed on the operating table with the legs straight or lithotomy position if female. The lithotomy position will allow the gynaecologists and assistant to work simultaneously and uterine manipulation would be possible. The thighs must not be flexed onto the abdominal wall as they would be in the full lithotomy position used for other open surgical gynecological procedures. The operating table is tilted head up or down by approximately 15 degree depending on the main area of examination. Compression bandage may be used on leg during the operation to prevent thromboembolism especially if patient is in lithotomy position.
Position of the Surgical Team Before starting diagnostic laparoscopy a best guess is made about the quadrant in which adhesion is more likely to be found. The surgeon should stand opposite to this quadrant to allow direct view into this quadrant. If the pathology is more likely in pelvic cavity the surgeon stands on left side of the patient. The first assistant, whose main task is to position the video camera, is also on the patient’s left side. The instrument trolley is placed on the patient’s left, allowing the scrub nurse to assist with placing the appropriate instruments in the operating ports. Television monitors are positioned on either side of the top end of the operating table at a suitable height for surgeon, anesthetists, as well as assistant to see the procedure.
Port PositionFor adhesiolysis of gynaecological purposes, generally one optical port in umbilicus and two 5 mm port in left and right iliac fossa should be introduced according to base ball diamond concept after visualizing the target of dissection. Port should be in a position to provide elevation angle of 30 degree and manipulation angle of 60 degree, which is ergonomically better. Some gynaecologist use suprapubic port, with suprapubic port, elevation angle of instrument and tubal structure is 90 degree and hence lifting up of ovary and tube may be difficult without grasping it.
Figure: Three ports for pelvic Adhesiolysis
A three-port approach should be used if there is any difficulty in manipulation with two ports especially in case of extensive adhesion.
· 10mm umbilical (optical)
· 5 mm suprapubic
· 5 mm right hypochondrium.
A 30° telescope is employed in most instances, as this facilitates easier inspection of the deeper peritoneal cavity and abdominal organs. The secondary ports are inserted under laparoscopic vision. The selected site on the abdominal wall is identified by finger indentation of the parietal peritoneum.
The open technique for trocar insertion is recommended if extensive adhesion is suspected. At the time of laparoscopic adhesiolysis, surgeon should try to be very gentle with the tubal structure and bowel so that re-adhesion will not form and stricture of tube will not occur.
Viewing of lateral pelvic organs is helped by the manipulation of mobile structure with a solid port introduced through the left iliac fossa port.
Laparoscopic Adhesiolysis
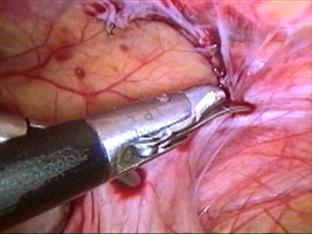
Figure: Sharp dissection with scissors for bowel adhesion
Animal studies have proved that laparoscopy leads to less adhesion formation compared to open surgery. The less adhesion formation after laparoscopic surgery is because retraction is not used much, packing of the abdominal cavity is not required that can damage peritoneum. In laparoscopic surgery there is less chance of drying of tissue because inside environment is cut off from outside. The foreign bodies like glove talk and lint. Also, the excellent visualization and magnification result into less tissue injury and adhesion. In laparoscopy, port wound and wound at the target of dissection is far away from each other so the chances of adhesion are less to the peritoneum because, for adhesion both the layer which tends to adhered should be in contact. At least three ports should be used to perform laparoscopic adhesiolysis. After access and introduction of telescope two other ports should be introduced according to baseball diamond concept keeping in mind the centre of adhesion as target of dissection.
Figure:Sharp dissection with scissors if bowel is involved
If the adhesion is thin and avascular, it is easily lysed and the chances of recurrence are not much. In contrast if adhesion is thick and highly vascular it is difficult to separate. Theses adhesion requires use of energy (Ultrasonic dissector, Unipolar or Bipolar). After achieving haemostasis sharp dissection with scissors are necessary.
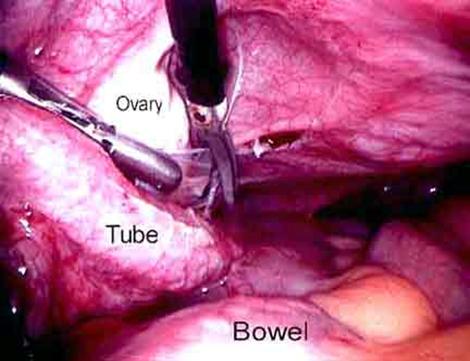
An atraumatic grasper is introduced to hold the adhesion or involved organ. It should be stretched gently and boundaries of adhesion are identified. An avascular area is choose with the close-up magnified view of telescope. The opposite trocar on the side of the surgeon is used for scissors and adhesion should be cut close to the affected organ. Vascular adhesions should be coagulated using electrosurgical instrument preferably, bipolar. Scissors should be used only if flimsy avascular adhesion is found. Thick vascular adhesion first should be tried with blunt dissection, otherwise must be coagulated before being cut. Suction irrigation instrument is good if blunt dissection is thought.
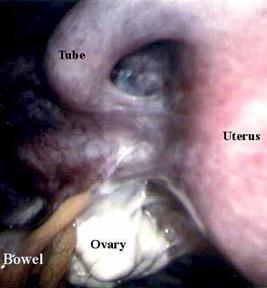
Figure: Tubo-ovarian mass with bowel involvement
Bowel injury is common during enterolysis and patient who have a history of previous laparotomy should undergo a bowel preparation. If Injury, results enterorrhaphy can be accomplished with a one layer closure using Vicryl. Details of intracorporeal suturing can be found in chapter of laparoscopic suturing and knotting.
After adhesiolysis some fluid can be left inside to prevent recurrence. Steroids and antihistamines were tried but are used infrequent because of adverse effect delayed wound healing and high risk of dehiscence.
High molecular weight dextran was tried to prevent re-adhesion because it is absorbed over a period of 7 to 10 day. Its osmotic effect draws the fluid into the peritoneal cavity and so the mobile peritoneal organ floats reducing adherence between intraperitoneal organs. Although study in animals has demonstrated reduced postoperative adhesion, it is not fully confirm for its efficacy.
Adhesion barrier membrane was also tried. These absorbable membrane separate peritoneal membrane from adhered organ and thus prevent fibrous bands from binding different structure. Two such materials are Interceed and Gore-Tex. Interceed is an absorbable fabric of oxidized regenerated cellulose, and Gore-Tex is nonabsorbable, nonreactive surgical membrane. Animal studies have demonstrated good result after using these membranes.

 因缺血而行小肠分段切除及一期吻合术
因缺血而行小肠分段切除及一期吻合术
 肌肉活检 _ 如何进行肌肉活检
肌肉活检 _ 如何进行肌肉活检
 尿道下裂修复后包皮瘘和龟头隐裂
尿道下裂修复后包皮瘘和龟头隐裂
 通过外部方法对喉囊肿进行有袋化或去顶
通过外部方法对喉囊肿进行有袋化或去顶

 发表于 2013-2-5 21:40:45
发表于 2013-2-5 21:40:45
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡










