马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
Problems due to Injury of Cysto-hepatic duct Prof. Dr. R. K. Mishra Cystohepatic duct Cystohepatic duct drains sub-segmental parenchymal distribution of right lobe of liver to the right hepatic duct or cystic duct. Problem occurs at the time of operation when it drains in Cystic duct. At the time of dissection this poorly visualized structure may go unnoticed. Injury results in bile leakage and patient may comes with complication even after 3 to 5 days after operation. Ducts of Luschka. Ducts of Luschka drains sub-segmental areas of liver into right hepatic duct. It is typically small in size, also called as subvesical duct. It runs in the submucosa of the posterior gallbladder wall & Gallbladder fossa. Complications after Overlooked Injury · If size of the duct is small enough leakage may be Inconsequential. · Mild leakage will lead to self limiting post operative bile peritonitis. · Moderate leakage leads to severe generalized peritonitis. · Massive leakage leads to severe peritonitis with bile spillage from port wound. · Moderate & massive leakage if not treated immediately patient may die due to shock of peritonitis. Prevention of Injury. · Knowledge of anatomy · Good vision. · Proper Irrigation. · Careful dissection. · Routine Intra-operative use of cholangiogram. Intra-operative treatment of injured duct. · Confirmation of diagnosis by repeated intra operative cholangiography for naked segment sign. · It should be clipped or ligated. · If Pedicle is small enough than it should be cauterized. Post-Operative Diagnosis of Injured duct. · Traditional exploratory laparotomy to ligate the duct and drain the sub hepatic space. · If the duct is small < 2mm in diameter than computerized axial tomography or ultrasound guided percutaneous drainage is effective. · Now a days endoscopic stent application is also effective mode of treatment. Why endoscopic stent is effective? · After stent application resistance of the sphincter of oddi is reduced. · Bile travel through the path of least resistance. · Stent can be applied on the same session at the time of diagnostic endoscopy. · Endoscopic retrograde cholangiography with placement of stent is effective and tolerated by patient. · The stent can be removed after 3 months after confirmation of closure. Conclusion It is estimated that 10% of people have an accessory ducts within triangle of Calot. Cystohepatic duct and duct of luschka is one of them. The actual prevalence of a luschka duct is unknown. So every Laparoscopic surgeon should be careful of it. | 
 腹腔镜下胆总管囊肿切除术及高级胆道重建术
腹腔镜下胆总管囊肿切除术及高级胆道重建术
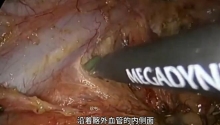
 机器人辅助腹腔镜胆囊次全切除术和胆总管探
机器人辅助腹腔镜胆囊次全切除术和胆总管探
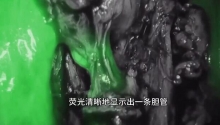
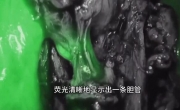 困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
 腹腔镜治疗85岁女性胆石性肠梗阻
腹腔镜治疗85岁女性胆石性肠梗阻

 发表于 2013-2-5 20:06:51
发表于 2013-2-5 20:06:51




 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡