马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
Laparoscopic versus Open Splenectomy Dr. Bayan H. Mohammed (DS, CABS, FRCSI), Consultant Surgeon. (Submitted as part of the requirement for DMAS study/World Laparoscopy Hospital/New Delhi/India) Abstract BACKGROUND: Laparoscopy is a relatively new surgical approach to excise the spleen as compared with the conventional open surgery. Many procedural and outcome factors are under continuous evaluation and others are still controversial. AIM: This review aims at highlighting the current view of laparoscopic Splenectomy as compared with the open Splenectomy. METHODS: A literature search performed using engine Google, High wire press, Springer link, and Yahoo. Selected papers screened for other related reports. RESULTS: Shorter hospital stay and reduced morbidity found to be clearly weighting on the side of laparoscopy, especially in normal and moderate size spleens. Introperative bleeding, operative time, though still more in the laparoscopic surgery but great advance reported due to the use of high technique instruments and adoption of new operative or preoperative procedures. CONCLUSION: Laparoscopic Splenectomy is a well-established and reliable procedure for spleens less than 20cm in length and has a less reported morbidity. The introduction of harmonic scalpel, preoperative embolization, morcellation and adoption of lateral approach are gradually eliminating the difficulties and more procedures that are laparoscopic are being done for larger spleens. KEY WORDS: Splenectomy, Laparoscopic Splenectomy, Open Splenectomy, Laparoscopic versus Open Splenectomy. INTRODUCTION:
Splenectomy is the surgical removal of the spleen. Traditionally, removal of the spleen accomplished by one large commonly a left subcostal or a left upper paramedian incision. The use of smaller incisions leads to less pain after surgery, less time spent in the hospital, and quicker return to work[1]. The first reported splenectomy done by zacarello in 1549 and O’ Brien in1816 in Europe and North America respectively. Laparoscopic Splenectomy i.e. the removal of the spleen through key hole incisions, is claimed to be associated with less postoperative pain, shorter hospital stay, and quicker return to normal activity and work. The earliest reports of Laparoscopic Splenectomy were published in the period between late 1991 and early 1992 by an independently working four groups, Delaître in Paris, Carroll in Los Angeles, Cushieri in the United Kingdom, and poulin et al in canada published the first reports of laparoscopic splenectomy in patients with hematologic disorders [2, 3, 4]. Since that time, the operative techniques for partial laparoscopic splenectomy was developed and put the limits of minimally invasive surgery under test until now where the technique of the operation is much simplified [5, 6]. Although, both operations, open and laparoscopic Splenectomy are essential components of splenic surgery, laparoscopic Splenectomy has led to a decrease in the indications for open approach.
Indications for splenectomy - Hereditary Spherocytosis. Is aa specific indication for laparoscpic Splenectomy. In HS, a specific protein in the red blood cell membrane is absent that leads to the formation of relatively fragile red blood cells that damage with increasing easiness when they pass through the spleen. This cell destruction occur nowhere in the body and ends when the spleen is excised.
- Splenic Carcinoma. Although reported, but it is a relative contraindication for laparoscopic approach due to the risk of dissemination.
- Idiopathic Thrombocytopenic Purpura. Immune (idiopathic) thrombocytopenic purpura (ITP). ITP is a disease of increased bleeding tendency due to platelet destruction by the spleen.Splenectomy reported to be the definitive treatment for this disease and is effective in around60 to 70% of chronic ITP patients.
- splenic trauma. Both blunt and penetrating trauma of the abdomen and lower chest can rapture the spleen alone or in association with other organs. Car accident blamed to be the commonest cause of blunt type of trauma. Trauma is regarded as a contraindication to laparoscopic Splenectomy.
- Hypersplenism. Is a syndrome rather than a specific disease. It consists of a group of symptoms that may be produced by a number of disorders. It characterizes by splenomegaly i.e. enlargement of the spleen, defects in one or more of the blood elements with high turnover of blood cells. Splenomegaly due to specific disorders like liver cirrhosis or certain cancers s commonly associated with hyper splenism.
- Miscellaneous conditions. These may include, Splenic Abscess, Raptured Splenic Artery, Thalassemia, Thrombotic Thrombocytopenic Purpura, Staging for Hodjkin’s disease, Myelofibrosis.
AIM: Is to highlight the currant situation regarding the feasibility, safety, of laparoscopic Splenectomy and to compare that with open Splenectomy in terms of size of spleen, operative time, peroperative bleeding and technical difficulties, finding of accessory spleen, and post operative morbidity. METHODS: A literature search performed using engine Google, High wire press, Springer link, and Yahoo. Selected papers screened for other related reports. Preoperative preparation: - Treatment of any concurrent infection.
- Correction of blood cell abnormalities.
- Patient should receive a polyvalent vaccine at least one to two weeks prior to surgery as prophylaxis against pneumococcal and meningococcal infection.
- Heparine may be given according to standard guidelines as a prophylaxis against thrombosis provided that there is no hematologic contraindication.
- Pre-emptive analgesia given, to minimize postoperative pain. However, Non-steroidal anti-inflammatory drugs not used when heparin prophylaxis is employed.
- Bowel preparation. Both mechanical and antibiotics against bowel flora are specially needed in most of the laparoscopic procedures.
Assessment of spleen volume:
The size of the spleen is usually measured by ultrasonography as expressed by the maximum crainiocuadal or interpole length (the length of the line joining the two poles of the spleen) (7). Computed tomography is indicated whenever there is doubt about ultrasonic measurement at the upper pole with spleens more than 16 cm. the size of the spleen is generally classified into three categories(8).
- Normal spleen size. The interpole length is < than 11 cm.
- Moderate splenomegaly. The interpole length is 11-20 cm.
- Sever splenomegaly. The interpole length is > than 20 cm.
Operative technique. 1. Laparoscopy.
Latral approach:
The technique of lateral approach was described in detail[10, 11].
This is currently used for most laparoscopic splenectomies [9]. At present, the anterior approach to laparoscopic splenectomy used for the excision of massive splenomegaly, which indicates an interpole length of more than 23cm or a 3 kg in weight.
1. Positioning of the patient and room setting : This is achieved by placing the patient in the right lateral decubitus position and to increase the distance between the lower margin of the thoracic cage and the iliac crest the operating table must be flexed and the kidney bolster elevated. Some surgeons prefer a slight tilt of the patient backward, and place the abdominal side of the patient nearer to the table edge. Room setting is: surgeon and camera operator stands on the right of the patient with the operator to the right of the surgeon. In consistence with coaxial alignment, the monitor is to the left of the patient. The mayo”s stand near the feet.
2. Insertion of trocars: Four 12 mm trocars usually introduced in the subcostal margin. By this the telescope, the clipper, and the linear stapler interchanged as needed taking into consideration a good distance between them to have a good working angles. Some surgeons prefer a slight tilt of the patient backward and place the abdominal side of the patient nearer to the table edge.
Although pneumoperitoneum created primarily through a veress needle, many surgeons prefer insertion of the primary trocar under direct vision to avoid the complications associated with the blind method, thought very small in number but more catastrophic than injuries associated with the open technique [1] A pneumoperitoneum started up to a pressure of 15mm Hg [1]. The second and third trocars inserted according to size and other anatomic factors of the spleen. In most cases, the fourth posterior trocar delayed until the splenic flexure of the colon has mobilized.
Variation in trocar placement may include using a three instead of four trocars and experienced surgeons may replace one or two 12 mm trocars by 5 mm one.
3. Exploration and excision of accessory spleens: This needs medial retraction of the stomach so that the spleen exposed.
The accessory spleens should be looked for in all the known locations and once found, an accessory spleen must be removed immediately since once stained with blood it will be difficult to relocate it. Accessory spleen excision is very important in ITP to prevent recurrence of the disease.
4. Mobilization of the lower pole: The splenocolic ligament incised to partially, mobilize the splenic flexure of the colon. An extension of the incision slightly to the left side of the gastrocolic ligament gives a window to the gastrosplenic ligament. This latter now separated from the splenorenal ligament. This step will give a view of what called the splenic tent. The left and right walls of this tent consist of the gastrosplenic and splenorenal ligaments respectively and the floor consist of the stomach i.e. the lesser sac now opened laterally.
By the use of electrocautery the branches of the gastroepiploic artery can be controlled otherwise application of a clips when these branches are large in size. The gastrosplenic ligament now incised between the gastroepiploic artery and the short gastric arteries. This portion is avasculr. A gentle retraction on the lower pole of the spleen at this stage will expose the hilar structures in the splenorenal ligament to assess the anatomy in this area to determine the level of difficulty and the need for a fourth trocar which can be inserted under vision posteriorly. Next the the phrenicocolic ligament should be incised up to the left crus of the diaphragm with the use of electrocautery leaving a small portion to help not only to suspend the organ but to help put it in the retrieval bag.
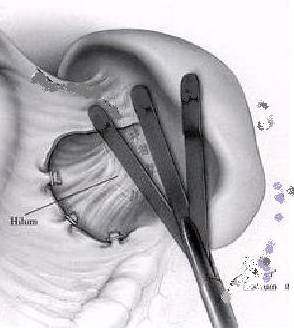
5. The splenic hilum: This depends much on the anatomy of the splenic vasculature. If they are of “distributed anatomy”, they can be dissected and clipped. On the other hand, a “bundled anatomy” dealt with by a single use of a linear stapler after identification of the tail of the pancreas. A window opened in the splenorenal ligament above the hilar pedicle help marking the ends of the stapler. The short gastric arteries taken in mass by the linear stapler or dissected and clipped. 7. Retrieval of the spleen: A medium or large size retrieval bag folded and introduced through one of the 12 mm trocars. When inside it should be unfolded and the spleen slipped inside gently to avoid splenosis, facilitated by keeping the upper pert of the phrenicosplenic ligament intact as described above which should be divided at this stage. Extraction done after a slight extension of the subcostal or umbilical incision. The bag edges held b a grasper inserted through the incision applying gentle traction will help in taking the spleen out to the surface. A suitable piece divided for biopsy, the spleen fragmented using the finger, and the blood sucked out. Repeating this help in extraction of the bag and the remaining part of the spleen. At the end, a second look taken to make sure of hemostasis, the abdomen deflated, trocars removed and the incisions closed with absorbable sutures. Anterior approach: The procedure is described elsewhere [11].
Currently this approach is preferred for some spleens between 21 and 30 cm (massive splenomegaly) and all spleens above 30cm or more than 3kg. Because large spleens are heavy and difficult to handle, a hand assisted laparoscopy using this approach is the operation of choice. Another indication, though relative, is if there is another abdominal operation to be done simultaneously like cholecystectomy.
1. Patient position and trocar placement: It is more comfortable for the surgeon to work between legs so the patient put in the modified lithotomy and steep fowler position with right tilt. This will also allow assistants to stand on each side of the patient. The primary 12mm port inserted through the umbilicus. Two secondary 12mm each are inserted each hypochondrium under vision. Another two 5mm trocars inserted just below the costal margin bilaterally. Another way of distributing the trocars is to put them in a semicircle away from the left hypochondrium.
2. Control of vascular pedicle:A hepatic retractor is passed through the right 12mm port to retract the left lobe of the liver, a step that help in pulling the stomach medially. Accessory spleens searched for and removed. Using electrocautery each of the phrenicocolic, splenocolic, and the sustentaculum lienis are incised as near as possible to the lower pole of the spleen. If vascular adhesions on the medial side of the spleen-a frequent finding- they should be cauterized. Next step is to dissect the gastrocolic ligament near the spleen; branches of the lef gastroepiploic artery ligated or clipped one by one or cauterized if small. To expose the splenic hilum and pancreatic tail within the splenorenal ligament, both upper and lower poles should gently lifted by two palpators introduced through two 5mm ports.
At this stage, the branches of the splenic artery and vein ligated or clipped nearer to the spleen. The devascularised portion of the spleen can be distinguished b change of their color from pink to grayish.
3. Extraction of the spleen: To put a massive or mega spleen (the usual indications for anterior approach) in a bag is very difficult and bags of that accommodate such size are not available. In these cases, an accessory incision for extraction is used. This may be a pfannenstiel incision or a left iliac fossa incision, though the first one considered to give a better cosmetics. If the spleen is difficult to extract, it should be put in the pelvic cavity and fragmented and the abdominal cavity copiously irrigated to prevent spleenosis.
open or conventional Splenectomy: due to the wide spread use of laparoscopic approach, the indications for open Splenectomy became narrow and limited to megaspleens and treatment of splenic trauma when conservative treatment is contraindicated or has failed.
1. Patient position and inscision:The supine position is used with a reverse trendelenburg and a 15 degree right tilt. A long upper midline incision that starts to the left of the xiphoid is used. This may later be extended according to the needs. An alternatively a left subcostal incision may be used for elective normal or small size spleens. An assistant on each side help retracting the abdominal wall and left lobe of the liver otherwise is to use a self-retaining retractor.
2. Exposure and ligation of splenic artery: The splenic artery located above the pancreas and this needs opening the lesser sac.
3. Mobilization of the spleen: A nasogastric tube in place, using the left hand the surgeon should retract the spleen anteromedially. The phrenicocolic ligament-now under stretch, incised from down upward and extended to the left crus of the diaphragm. The left lateral part of the gastrocolic ligament dissected now to mobilize the spleen. What remain at this step are the splenocolic ligament and the sustentaculum lienis only. A gentle finger dissection between the pancreas and retroperitoneal structures will help to deliver the spleen to the midline.
4. Resection of the spleen: What remains of small blood vessels divided between curved clamps and ligated starting from the lower pole. Post operative care:
This is almost similar in both laparoscopic and open methods. It consist of removal of nasogastric tube either immediately postoperatively or in the recovery room, taking into consideration that in children this ma be delayed more due to more frequent postoperative gastric dilatation. Urinary catheter if placed should be removed after finishing the operation. Post operative analgesia given according to the general guidelines.
Results:
1. Operative time: Although many surgeons report on a longer overall, operative time for laparoscopic approach and the difference was significant but this was affected by many other factors.
2. Postoperative hospital stay: This was shorter in the laparascopic groups and it was sometimes significant.
3. Intraoperative bleeding: No significant difference in operative bleeding found between both groups.
4. Missing of accessory spleen(s): is significantly more in laparoscopic vs open Splenectomy, though a better figures are observed with lateral approach.
5. Morbidity: This was found to be less in the laparoscopic patients. Postoperative pain was not prolonged and the dose and duration for opiate was reduced. postoperative oral intake initiated earlier. Discussion: In surgical practice, the greater part of morbidity is due to the wounds through which the target organ dissected and removed. Many examples given in every day surgical work, like cholecystectomy wher the operative procedure is the same and the only difference is the access. Predicting that post operative morbidity minimized, encouraged laparoscopic Splenectomy as is clearly shown by being one of the earliest solid-organ procedures. This encouraging projection was confirmed by many of the early reports [1, 12, 13, 14,
And 15]. Then many comparative studies started to emerge regarding the differences, though unlikely to be major, which may exist between open and laparoscopic approaches in terms of feasibility and perioperative morbidity [16, 17, and 18]. Points of comparison include time of operation, blood loss, length of hospital stay and morbidity.
Although many reports showed a significant results for longer operative time in laparoscopic than open Splenectomy[19, 20, 21, 24, 25], but this difference was more clear when laparoscopic Splenectomy was done for super massive spleens and when Splenectomy was done for blood malignancy [21,22,24,26]. On the other hand many authors report a shortened operative time in normal and small spleens, and when using harmonic knife [21, 24]. This may encourage a more adoption of laparoscopic splenectomies as in medical instrument engineering will provide a more advances.
Shortened hospital stay reported by many authors and is the most obvious advantage of laparoscopic Splenectomy [20, 21, and 22]. This observation seen clearly in patients older than 65 years when compared with open laparoscopy for the same age group. This may suggest the better catabolic response in laparoscopy especially in this age group [16]. Although the learning curve ascension is successful, laparoscopic Splenectomy has still longer operative time vs open one. This is explained by time needed for patient positioning, pneumoperitonium to be established, and retrieval of the organ. On the other hand, many authors report some shortening in operative time due to factors like improvement of instruments used like the harmonic knife [23].
The second point of comparison was the intraoperative bleeding. It was found that bleeding is slightly more in laparoscopic patients than open one but the difference was insignificant. Many authors found that this increased loss of blood is more when operating on large spleens (more than 15cm) vs small, and malignant vs benign[24,26]. On the other hand a decease in the amount of blood lost can be achieved with improvement of learning curve, early ligation of splenic artery, preoperative splenic artery embolization, and improved technology like the use of harmonic knife [25, 28, 29, 30].
Missing an accessory spleen was another point of criticism [16, 18, and 30]. Surprisingly, the published incidence of missed accessory spleen(s) in splenectomised patients for hematological disease is 10%-20% as compared to 4.8% in open cases [15, 16, and 22]. The common anatomic area where these may be found in order of frequency are: splenic hilum, gastrocolic ligament, pancreatic tail, greater omentum, greater curvature, splenocolic ligament, small and large bowel mesentery, left broad ligament, and left spermatic vein in men[30]. Most of these sites are better seen in the lateral approach [22].
Postoperative pain is mainly due to somatic trauma as compared to visceral trauma. In laparoscopic surgery, there is minimal trauma and dissection of the abdominal wall due to the use of small wounds i.e. a minimum access. Many authors report less postoperative pain and a decreased need for opiate in terms of dose and duration. On the other hand, the duration of parenteral hydration was shortened and early resumption of oral diet achieved [25].
Another clear difference between laparoscopic vs open laparoscopy is the probably unreported occurrence of wound infection, pneumonia and subphrenic abscess after laparoscopic splenectomy [27, 28, and 31]. This may be explained by a less disturbance of the internal milieu and less suppression of the immune function than after laparotomy [22]. CONCLUSION: Laparoscopic Splenectomy is safe procedure, is feasible at present time for spleens less than 20cm length, and is associated with better postoperative morbidity. Laparoscopic operations for larger spleens are on the increase. This is due to use of preoperative splenic artery embolization and the availability of high technology instruments. References 1. Eric C. Poulin, MD, MSC, FACS, FRCSC. Joseph Mamazza, MD, FRCSC. Christopher M. Schlachta, MD, FACS. 5 Gastrointestinal Tract and Abdomen, 25 Splenectomy, ACS Surgery Online, Dale DC; Federman DD, Eds. WebMD Inc., New York, 2000.
2.. Delaitre B, Maignien B: Splénectomieparvoielap aroscopique, 1 observation. Presse Médicale 20:2263, 1991.
3. Carroll BJ, Phillips EH, Semel CJ, et al: Laparoscopic splenectomy. Surg Endosc 6:183, 1992.
4. Thibault C, Mamazza J, Létourneau R, et al: Laparoscopic splenectomy: operative technique and preliminary report. S urg Laparosc Endosc 2:248, 1992.
5. Poulin EC, Thibaul C, DesCôteaux JG, et al: Partial laparoscopic splenectomy for trauma: technique and case report. Surg Laparosc Endosc 5:306, 1995.
6. Seshadri PA, Poulin EC, Mamazza J, et al: Technique for laparoscopic partial splenectomy. Surg Laparosc Endosc 10:106, 2000.
7. Lewis J Kaplan, MD, FACS, David Coffman, MD, Splenomegaly
8. Goerg C, Schwerk WB, Goerg K, et al: Sonographic patterns of the affected spleen in malignant lymphoma. J Clin Ultras ound 18:569, 1990.
9. Gagner M, Lacroix A, Bolte E, et al: Laparoscopic adrenalectomy: the importance of a flank approach in the lateral decubitus position. Surg Endosc 8:135, 1994
10. Park A, Gagner M, Pomp A. Laparoscopic splenectomy: superiority of the lateral approach. Abstract presented at: Annual Meeting of the Royal College of Physicians and Surgeons of Canada; September 8, 1993; Vancouver, British Columbia.
11. Park A, Gagner M, Pomp A. The lateral approach to laparoscopic splenectomy. Am J Surg. 1997;173:126-130.
12. Delaitre B, Maignien B, Icard P. Laparoscopic splenectomy [letter]. Br J Surg. 1992;79:1334.
13. Caroll BJ, Phillips EH, Semel CJ, et al. Laparoscopic splenectomy. Surg Endosc. 1992;6:183-185.
14. Hashizume M, Sugimachi K, Ueno K. Laparoscopic splenectomy with an ultrasonic dissector [letter]. N Engl J Med. 1992;327:438.
15. Glasgow RE, Yee LF, Mulvihill SJ. Laparoscopic splenectomy: the emerging standard. Surg Endosc. 1997;11:108-112.
16. Brunt LM, Langer JC, Quasebarth MA. Comparative analysis of laparoscopic versus open splenectomy. Am J Surg. 1996;172:596-601.
17. Hashizume M, Ohta M, Kishihara F, et al. Laparoscopic splenectomy for idiopathic thrombocytopenic purpura: comparison of laparoscopic surgery and conventional open surgery. Surg Laparosc Endosc. 1996;6;129-135.
18. Watson DI, Coventry BJ, Chin T, Gill PG, Malycha P. Laparoscopic versus open splenectomy for immune thrombocytopenic purpura. Surgery. 1997;121:18-22.
19. Owera A; Hamade AM; Bani Hani OI; Ammori BJLaparoscopic versus open splenectomy for massive splenomegaly: a comparative study.J Laparoendosc Adv Surg Tech A. 2006; 16(3):241-6 (ISSN: 1092-6429).
20. M. Trias, E. M. Targarona and C. Balagué.laparoscopic splenectomy: an evolving technique..Surgical Endoscopy.Volume 10, Number 4 / April, 1996.
21. Rosen M, Brody F, Walsh RM, Tarnoff M, Malm J, Ponsky J.Outcome of laparoscopic splenectomy based on hematologic indication.Surg Endosc. 2002 Feb;16(2):272-9
22. Friedman RL, Fallas MJ, Carroll BJ, et al. Laparoscopic splenectomy for ITP: the gold standard. Surg Endosc. 1996;10:991-994.
23. Sapucahy Manuela V. ; Faintuch Joel ; Bresciani Cláudio J.C. ; Bertevello Pedro L. ; Habr-Gama Angelita ; Gama-Rodrigues Joaquim José. Laparoscopic versus open splenectomy in the management of hematologic disease.Revista do Hospital das Clínicas. 2003; 58(5):243-249
24. Adrian Park, MD; Michael Marcaccio, MD; Marion Sternbach, MD; Donald Witzke, PhD; Peter Fitzgerald, MD. Laparoscopic vs Open Splenecto. Arch Surg. 1999;134:1263-1269.
25. Rothenberg SS.Laparoscopic splenectomy using the harmonic scalpel.: J Laparoendosc Surg. 1996 Mar;6 Suppl 1:S61-3.
26. Pugliese R; Maggioni D; Scandroglio I; Sansonna F; Grilloa G; Di Lernia S; Ferrari GC; Boniardi M; Costanzi A; Magistro C. Splenectomy in haematologic diseases. Clinical indications and surgical technique]Chir Ital. 2005; 57(3):283-91.
27. Owera A; Hamade AM; Bani Hani OI; Ammori BJ.Laparoscopic versus open splenectomy for massive splenomegaly: a comparative study.J Laparoendosc Adv Surg Tech A. 2006; 16(3):241-6 .
28. Poulin EC, Thibault C, Mamazza J. Laparoscopic splenectomy. Surg Endosc. 1995;9:172-177.
29. Asoglu O, Ozmen V, Gorgun E, Karanlik H, Kecer M, Igci A, Unal ES, Parlak M.Does the early ligation of the splenic artery reduce hemorrhage during laparoscopic splenectomy?.Surg Laparosc Endosc Percutan Tech. 2004 Jun;14(3):118-21.
30.Palanivelu C, Jani K, Malladi V, Shetty R, Senthilkumar R, Maheshkumar G.
Early ligation of the splenic artery in the leaning spleen approach to laparoscopic Splenectomy. J Laparoendosc Adv Surg Tech A. 2006 Aug;16(4):339-44
.31.Gigot J-F, Lengele B, Gianello P, et al. Present status of laparoscopic splenectomy for hematologic diseases: certitudes and unresolved issues. Semin Laparosc Surg. 1998;5:147-167. |

 腹腔镜胆囊切除术中胆囊动脉出血的处理
腹腔镜胆囊切除术中胆囊动脉出血的处理
 MAGPI 尿道下裂修复
MAGPI 尿道下裂修复
 腹腔镜胆囊切除术
腹腔镜胆囊切除术
 坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
坏疽性胆囊 - 腹腔镜胆囊切除术及技巧

 发表于 2013-2-4 19:06:03
发表于 2013-2-4 19:06:03

 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡