马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
LAPAROSOPIC VERSUS OPEN MANAGEMENT OF HYDATID CYST OF LIVER
Dr. Anna Grazia Sabelli
Consultant Surgeon
Milano Italy P.O. Box 20154
Milano Milano
20154 Italy Project submitted towards completion of Diploma in Minimal Access Surgery, World Laparoscopy Hospital, India 110018 Abstract: Background: To compare laparoscopic versus open management of the hydatid cyst of the liver
Methods: Searching Medline, EMBASE, Springer link , Google to analyze: Surgical procedures and Complications Keywords:
Laparoscopical treatment of liver cyst, laparoscopic approach to abdominal hydatid cyst Introduction:
Echinococcosis is caused by the metacestode of Echinococcus species. The majority of Echinococcus infections are due to: Echinococcus granulosus and Echinococcus multilocularis. This zoonotic infection is mainly endemic in Mediterraneon countries, in Middle East and Africa whereabouts exist travels and immigration. The most common site of occurrence of hydatid cyst in the humans, that are accidental intermediate host, is the liver ( from 50 to 70% ). Surgical management must take morphology, size, situation and number of cysts into account . Different surgical procedures have been suggested and compared, but our interest regards: - Open procedure
- Laparoscopic treatment
Both treatments for selecting operative cases helps to appropriate morphologic classifications. Trought Gharbi classification by abdominal ultrasonography and computed axial tomography it is possible distinguish unilocular (Gharbi type I and II ), multilocular ( Gharbi type III ) and degenerated ( Gharbi type IV ) cysts.
The WHO ( World Health Organization ) proposed a new classification evaluating the functional state of the parasite that facilitate selection of treatment modalities.
WHO classification: | Type of cyst | Status | Ultrasound features | Remarks | | CL | Active | Signs not pathognomonic, unilocular, no cyst wall | Usually early stage fertile differential diagnosis necessary | | CE 1 | Active | Cyst wall, hydatid sand | Usually fertile | | CE2 | Active | Multivescicular, cyst wall, “rosette like” | Usually fertile | | CE3 | Transitional | Detachment of laminated membrane, “water lily sign”. | Starting to degenerate | | CE4 | Inactive | Less round-decreased intracystic pressure Heterogeneous hypo- or hyper- echogenic degenerative Usually no living ptotosco contents; no daughter cysts | May produce daughter cysts differential diagnosis necessary | | CE5 | Inactive | Thick calcified wall, calcification partial to complete; Usually no living | Not pathognomonic but highly suggestive of protoscolices |
Syntoms: - Right upper quadrant pain
- Nausea and vomiting
- Right abdominal tenderness
- Jaundice
- Allergic reactions
Diagnosis: The diagnosis is established by ultrasonography and computed axial tomography; in doubtful are undertaken immunological tests and detection of anti-echinococcal antibodies. Particular technique called ELISA ( Enzyme Linked Immuno Sorbent Assay ) have a high specificity and accuracy. Tecniques: Open Surgery Procedures: The open conservative approach is applied for giant cysts and consists of: neutralization of the parasite, evacuation of cystic components, treatment of the pericystic cavity and management of cist-bile duct communications if present.
In the surgical simple drainage the abdomen is protected with gauze packs around the cyst to reduce the peritoneal contamination risk. Once aspirated, the cavity is sterilized with antiscolecoidal agents ( e.g. abendazole, hipertonic solutions ) and the cyst is unroofed and drained.
Marsupialization and capitonnage procedures are not use anymore because of the high complications rate.
There are more aggressive operations how hepatectomy and total pericystectomy that often cause immunologic reactions, infection of hepatic parenchyma and postoperative bile leakage. Indications: - Single superficial cyst that may rupture
- Large cyst with multiple daughter cysts
- Cysts in communication with the biliary tree
- Infected cysts
- Cysts giving compression to the near vital organs
Controindications: - Dead cysts
- Multiple cysts
- Cysts difficult to access
- Small cysts
Laparoscopic Procedure: Although there aren’t randomized clinical trials comparing laparoscopic versus open surgical treatments, more and more, in the last fifteen years laparoscopic management of liver echinococcosis has gain ground producing encouraging results. Palanivelu planned a recent technique, the so-called PHS ( Palanivelu Hydatis System. The PHS consists of a complex system of fenestrated trocar and cannulas through wich it’s reduced at least the peritoneal spillage). Controindications: - Deep intraparenchimal cysts
- Posterior Cyst
- More than 3 cysts
- Cysts with tick and calcified walls.
- Cysts characterized by heterogeneous complex mass ( Gharbi type 4 )
- Cyst less than 3 cm in diameter
- Serious coagulation abnormalities
Technique: After creating of pneumoperitoneum through the umbilicus and after identifying the hydatid cyst, the PDS trocar is introduced into the peritoneal cavity directly over the hydatid cyst. Once the trocar is removed only the cannula is advanced until its tip is in contact with the hydatid cyst surface. After suction with cannula, a 5 mm trocar jointed to another suction machine is introduced into the cannula and is pushed into the cyst. The suction is immediate and happens either into the body of the hollow trocar and into the suction cannula, or into cannula and then into the suction side-channel.
The trocar is removed, the peritoneal cavity is irrigated by the main channel while the suction is maintained all the time. After removing fluid, the telescope is introduced to visualize the interior of the cavity for control any cyst-biliary communication; a scolicidal agent is instilled into the cyst cavity and after 10 minutes it is suctioned and the cyst is marsupialized. In case of bile leakage use of scolicidal agent is avoided for the cholangitis risk. Omentoplasty is done in all case and a drainage tube is put near the cyst. Complications: The most common complication is the creating of external biliary fistula ( 5-25% ). Some authors suggest a conservative therapy when the daily bile output is < 300 ml replacing the patient’s daily fluids and electrolyte losses. For high –output fistulas > 300 ml more than 1 week duration and low-output fistulas of more than 3 weeks duration were treated by endoscopy sphinterotomy.
Other immediate complications can be anaphylactic shock due to spillage caused during puncture cyst maneuver, bleeding and post-operative infection with creating of perihepatic abscesses. A later complication is the recurrence; the rate of short-time recurrence ( by some authors ) varies from 0% to 9% after laparoscopy, it is higher in open ( 0% to 30% ). Discussion: The choice of the better management of hydatid cyst of the liver is very difficult because of variable clinic-pathologic aspects. The treatment should be individualized to the morphology, size, number and location of the cysts. The progresses fulfilled in the latest years by laparoscopic management have made the applications of this technique possible to a number more and more growing of cases. It is sure that the Palanivelu Hydatid System ( PHS ) have revolutionized the treatment of hydatid cyst of the liver because its sealed procedure not only avoids any spillage of the fluid , but also allows intracystic magnified visualization for cyst biliary communications. By its application field are excluded only deep intraparenchymal or posterior cysts situated close to the vena cava. Consequently it is reduced time range hospitalization that is for the laparoscopy, in the opinion of some authors, of 3-12 day against the mean hospitalization time range in the open that is of 9-20 days; mortality with the laparoscopic procedure goes down almost 0% as morbidity as that has determinate a dramatic and sensible reduction of the recurrence References:
[1] A. Bickel, G. Daud, D. Urbach, E. Lefler, EF Barash, A. Eitan. Laparoscopic approach to hidatid liver cyst. Is it logical? Physical, experimental an practical aspects. J Surgical Endoscopy Vol 12 n 8 1998
[2] A. Bickel, N. Loberant, J. Singer- Jordan, M. Goldfeld, A. Eitan. The laparoscopic Approach to abdominal Hydatid Cysts. Arch. Surg./Vol. 136, 2001
M. Ertem, T. Karahasanoglu, N. Yavuz, S. Erguney. Laparoscopically Treated Liver Hydatid Cysts. Arch. Surg. 137: 1170-1173. 2002
[3] C. Kayaalp. Evacuation of Hydatid Liver Cysts Using Laparoscopic Trocar. World J. Surg. 26, 1324-1327. 2002
[4] G. Skroubis, C. Vagianos, A. Polydoron, E. Troracoleftherakis, J. Androulakis. Significance of Bile Leaks Complicating Conservative Surgery for Liver Hydatidotis. World J. Surg. 26, 704-708. 2002
[5] F. Giuliante, F. D’Acapito, M. Vellone, I. Giovannini, G. Nuzzo. Risk for Laparoscopic fenestration of Liver Cysts. Surg. Endosc. 17: 1735-1738. 2003
[6] C. Dervenis, FRCS, S. Delis, C. Augerinos, J. Madariaga, M. Milicevic. J. Gastrointest. Surg. 9: 869-877. 2005
[7] M. Kapan, S. Kapan, E. Goksoi, S. Perek, E. Kol. Postoperative recurrence in hepatic hydatid disease. J Gatrointest. Surgery 2005
[8] C. Palanivelu, K. Jani, V. Malladi, R. Senthilkumar, PS Rajan, K. Sendhilkumar, R. Parthasarthi, A. Kavalakat | 
 腹腔镜下胆总管囊肿切除术及高级胆道重建术
腹腔镜下胆总管囊肿切除术及高级胆道重建术
 机器人辅助腹腔镜胆囊次全切除术和胆总管探
机器人辅助腹腔镜胆囊次全切除术和胆总管探
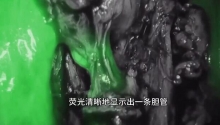
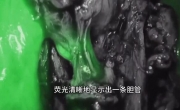 困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
 腹腔镜治疗85岁女性胆石性肠梗阻
腹腔镜治疗85岁女性胆石性肠梗阻

 发表于 2013-2-3 22:59:08
发表于 2013-2-3 22:59:08
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡