马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
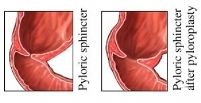
Pyloroplasty Pyloroplasty Definition Pyloroplasty is really a surgical treatment where the pylorus valve in the lower part of the stomach is cut and resutured, soothing and widening its muscular opening to the duodenum. Pyloroplasty is really a treatment for patients at high-risk for gastric or peptic ulcer disease (PUD). Purpose Pyloroplasty surgery makes bigger the opening by which contents of the stomach are emptied to the intestine, enabling the stomach to empty faster. A pyloroplasty is conducted to deal with the problems of PUD or when treatment is not in a position to control PUD in high-risk patients. Who performs the process and where could it be carried out? A pyloroplasty surgery is conducted with a general surgeon inside a hospital or clinic operating room. Demographics About 1.7% of kids receiving treatment generally pediatric practices are identified as having PUD. The existence of ulcer-causing Helicobacter pyloribacteria happens in 10% from the population in developed countries and it is thought to cause 80-90% of primary ulcers. The regularity of secondary ulcers isn't referred to as this will depend about the frequency of other illnesses, chronic diseases, and drug use. Primary and secondary PUD may appear in patients spanning various ages. Primary PUD is uncommon in younger patients under age 10, growing during adolescence. Secondary PUD is much more prevalent in younger patients under age six. Diagnosis Diagnosis starts with a precise good reputation for prior illnesses and existing health conditions in addition to a genealogy of ulcers or another gastrointestinal disorder. An entire background and comprehensive diagnostic testing can sometimes include: - heart rate, pulse, and blood pressure level
- bowel habits and outline of stool
- family and social stressors
- location, frequency, duration, and harshness of pain
- vomiting and outline of gastric material
- rectal examination and stool testing
- all medicines, which includes over-the-counter products
- appetite, typical diet, and weight changes
- urinalysis
- alcohol consumption and smoking habits
- chest examination and x ray, if required
- palpation from the abdomen
- examination of testicles and inguinal area in males
- pelvic examination in if perhaps patient are females
- testing for that presence of Helicobacter pylori
- complete blood count and blood chemistry profile
- imaging studies of gastrointestinal system (x-ray, other forms of scans)
Description Peptic ulcer disease evolves if patient find an imbalance between regular problems that protect the liner from the stomach and also the intestines and scenarios that disrupt regular functioning from the lining. Protective factors range from the water-soluble mucosal gel layer, producing bicarbonate within the lining to balance acidity, the unsafe effects of gastric acid secretion, and blood circulation within the lining. The aggressive factors that actually work from this protective gastric-wall system are extreme acid production, H. pylori infection, along with a reduced blood circulation within the mucosal lining. These aggressive factors may cause inflammation and ulcer advancement. A peptic ulcer is a kind of sore or hole that forms about the lining from the stomach or intestine, once the lining continues to be eaten away by gastric acid and digestive juices. Peptic ulcers could be primary, brought on by H. pylori infection, or secondary, brought on by excess acid production, stress, utilization of medicines, along with other underlying problems that disrupt the gastric environment. Although H. pylori is thought to make the most of all ulcers, not every people have contracted it grow ulcers. In high-risk individuals, the bacteria more easily disturb the total amount between good factors and destructive factors, upsetting the protective function from the stomach and intestine lining. An ulcer evolves once the lining can't protect the organs. Secondary ulcers are often based in the stomach; primary ulcers could be within the stomach or intestine. Additional factors that bring about mucosal inflammation and ulceration include: - cigarette smoking
- exposure to a particular irritating chemicals
- respiratory failure
- alcohol and caffeine use
- critical illnesses that creates imbalances in body
- non-steroidal anti-inflammatory drugs (NSAIDs)
- aspirin
- emotional disturbances and long term stress
- traumatic injuries and burns
- blood poisoning
The signs of gastric or peptic ulcer consist of burning pain, nausea, vomiting and lack of appetite, bloating, burping and slimming down. When PUD is diagnosed or high-risk is established, treatment will start to treat H. pylori infection if present and also to restore well balanced condition within the mucosal lining. Any underlying condition might be treated concurrently, such as respiratory disorders, fluid imbalance, or stomach and digestive complaints. Medicines might be prescribed to assist correct gastric disturbances and manage gastric acid secretion. Certain drugs which are prescribed for other problems, especially NSAIDs, might be discontinued when they are recognized to cause inflammation. Adult patients might be advised to stop alcohol and caffeine use and also to quit smoking. When treatment alone can't enhance the conditions that create PUD, a pyloroplasty procedure might be recommended, particularly for patients with stress ulcers, perforation from the mucosal wall, and gastric outlet obstruction. The surgery requires cutting the pylorus lengthwise and resuturing it in a right angle over the cut to unwind muscle that will create a bigger opening in the stomach to the intestine. The increased opening enables the stomach to empty faster. A pyloroplasty may also be completed in addition to a vagotomy procedure where the vagus nerves that stimulate gastric acid production and gastric movement are cut. This might delay gastric emptying and pyloroplasty can help factual that effect. Important questions patient should ask a doctor: - How will this surgery be practiced?
- What is the knowledge about this process?
- How frequently would doctor perform this process?
- Why should the patient undergo the surgery?
- What are the options basically opt not have access to the surgery?
- How can one be prepared to feel after surgery?
- What would be the risks involved with having one of these surgery?
- How quickly is a patient going to recover?
- When can one go back to school or work?
- What is my likelihood of getting this problem again?
- What should one do to avoid getting this problem again?
Preparation Before surgery, standard preoperative blood and urine tests are going to be performed as well as other x-rays might be ordered. The individual won't be permitted to consume or drink anything after midnight the night time prior to the procedure. Once the patient is admitted at the hospital, cleansing enemas might be ordered to empty the intestine. If nausea/vomiting exist, a suction tube enables patient to empty the stomach. Risks Potential difficulties of the abdominal surgery consist of excessive bleeding, surgical wound infection, and incisional hernia, repetition of gastric ulcer, chronic diarrhea, and malnutrition. Following the surgery, the doctor ought to be informed of the rise in pain, as well as any swelling, redness, drainage, or bleeding within the surgical area. The advancement of headache, muscle aches, dizziness, fever, abdominal swelling or pain, constipation, nausea / vomiting, rectal bleeding, or black stools also needs to be reported. Normal results Complete healing is anticipated without problems. Recovery along with a go back to normal activities should originate from 4 to 6 weeks. Morbidity and mortality rates Successful treating of Helicobacter pylori has enhanced morbidity and mortality rates, and also the prognosis for PUD, with medicine and prevention of causative factors, is great. Pyloroplasty is hardly ever performed in primary ulcer disease. Morbidity and mortality are higher in patients with secondary ulcers due to underlying illness that reduces both PUD and surgical procedure. Aftercare The individual will expend hours inside a recovery area after surgery where blood pressure level, pulse, respiration, and temperature is going to be monitored. The patient's breathing might be shallower than usual due to the effect of anesthesia and also the patient's desire not to breathe deeply and experience pain to begin from the surgical incision. The individual is going to be shown how patient can offer the site while breathing deeply or coughing, and patient will be given pain medicine when needed. Fluid intake and output is going to be measured. The operative site is going to be observed for any sign of redness, swelling, or wound drainage. Intravenous fluids are often given for 24-48 hours before patient is progressively permitted to consume a unique light diet so that as bowel activity resumes. About 8 hours after surgery, the individual might be permitted to walk just a little, growing movement gradually within the next 3 days. The typical hospital stay, based mostly on the patient's all round recovery status and any underlying circumstances, ranges from 6 to 8 days.
| 
 因缺血而行小肠分段切除及一期吻合术
因缺血而行小肠分段切除及一期吻合术
 肌肉活检 _ 如何进行肌肉活检
肌肉活检 _ 如何进行肌肉活检
 尿道下裂修复后包皮瘘和龟头隐裂
尿道下裂修复后包皮瘘和龟头隐裂
 通过外部方法对喉囊肿进行有袋化或去顶
通过外部方法对喉囊肿进行有袋化或去顶

 发表于 2013-2-2 17:21:42
发表于 2013-2-2 17:21:42
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡










