马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
Vagotomy Vagotomy Definition Vagotomy might be the surgical cutting from the vagus nerve to lessen acid secretion within the stomach. Purpose
The vagus nerve trunk divides into branches which go to various areas of the stomach. Stimulation from all of these branches results in the stomach to create acid. An excessive amount of gastric acid results in ulcers that could ultimately bleed that will create an urgent situation. A vagotomy is conducted when acid production within the stomach can't be decreased by other means. The objective of the process is to disable the acid-producing capacity from the stomach. It's used when ulcers within the stomach and duodenum don't react to medicine and alterations in diet. It's an appropriate surgery when patient will find ulcer difficulties, for example blockage of digestive flow, bleeding, or perforation. The regularity that elective vagotomy is conducted has decreased previously two decades since it is becoming clear how responsible for ulcers is definitely an infection with a bacterium called Helicobacter pylori. Drugs have grown to be increasingly effective for ulcers. However, the amount of vagotomies executed in emergency circumstances has always been comparable. A vagotomy procedure is usually performed along with another gastrointestinal surgery, for example partial elimination of the stomach (antrectomy or subtotal gastrectomy). Description A vagotomy can be carried out using closed (laparoscopic) or open surgical technique. The symptoms for any laparoscopic vagotomy overlap with open vagotomy. Patient will find four basic kinds of vagotomy procedures: - Selective (total gastric) vagotomy: The primary vagal trunks are dissected enough where the branch resulting in the biliary tree divides, and there's a cut in the portion of vagus near to the hepatic branch. This process is hardly ever pointed out or performed.
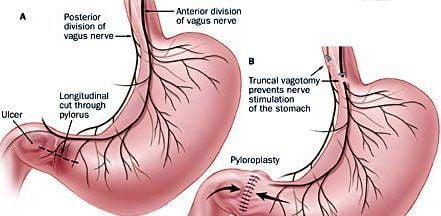
- Truncal or total abdominal vagotomy: The primary vagal trunks are divided, and surgery is along with a drainage procedure, for example pyloroplasty.
- Thoracoscopic vagotomy: Carried out with the third, sixth, and seventh left intercostal spaces, the posterior vagus trunk is isolated, clipped, along with a segment excised.
- Highly selective vagotomy (HSV): HSV selectively deprives the parietal cells of vagal nerves, and lessens their sensitivity to stimulation and also the discharge of acid. It doesn't need a drainage procedure. The limbs of Latarjet's nerve are divided in the esophagogastric junction towards the crow's foot across the lesser curvature from the stomach.
A vagotomy is conducted under general anesthesia. The surgeon bakes an incision within the abdomen and locates the vagus nerve. Either the trunk or even the branches resulting in the stomach are cut. The stomach muscles are sewn together again and also the skin is closed with sutures. Often, other gastrointestinal surgery is conducted simultaneously. Vagotomy leads to a reduction in peristalsis, along with an alternation in the emptying patterns from the stomach. To help ease this, a pyloroplasty is usually carried out to widen the outlet in the stomach towards the small intestine. Demographics Gastric ulcers are involved underneath the general heading of gastrointestinal (GI) diseases. GI disorders affect approximately 25%-30% from the world's population. Not treated, these conditions often develop into ulcers. 4 times as numerous duodenal ulcers as gastric ulcers are diagnosed. The first-degree relatives of patients with duodenal ulcer have 2 to 3 times’ the upper chances of establishing duodenal ulcer. Relatives of gastric ulcer patients possess a similarly enhanced risk of creating a gastric ulcer. Who performs the process and where could it be carried out? Patients who get vagotomies are generally observed in emergency circumstances where bleeding and perforated ulcers need immediate intervention. A vagotomy is generally performed with a board-certified surgeon, whether general surgeon who focuses on gastrointestinal surgical procedures or a gastrointestinal endoscopic surgeon. The process is performed inside a hospital setting. Diagnosis/Preparation A gastroscopy and x-rays from the gastrointestinal system figure out the positioning and condition from the ulcer. Standard preoperative blood and urine tests are carried out. The individual discusses using the anesthesiologist any medicines or conditions that may get a new administration of anesthesia. Questions a patient should ask a doctor: - What would be the possible problems involved with vagotomy surgery?
- What surgical preparation is required?
- What kind of anesthesia is going to be used?
- How will be the surgery carried out?
- What is the period of hospitalization?
- How many vagotomies does the doctor perform each year?
Risks Standard surgical risks, for example extreme bleeding and infection, are potential problems. Additionally, the emptying patterns from the stomach are changed. This may lead to dumping syndrome and diarrhea. Dumping syndrome is really a symptom in that the patient experiences palpitations, sweating, nausea, cramps, vomiting, and diarrhea soon after eating. The next problems will also be related to vagotomy surgery: - Gastric or esophageal perforation. May take place from an electrocautery injury or by clipping the branch from the nerve of Latarjet.
- Delayed gastric emptying. Most typical after truncal and selective vagotomy, especially if a drainage procedure isn't done.
Individuals who use alcohol too much, smoke, are obese, and therefore are very young or aged are in greater risk for problems. Normal results Normal recovery is anticipated for many patients. Ulcers recur within 10% of those that have vagotomy without stomach removal. Recurrent ulcers will also be present in 2%-3% of patients who've some part of their stomach eliminated. Aftercare Patients who may have had a vagotomy remain in a healthcare facility for around 7 days. Nasogastric suctioning is needed for that first 3 or 4 days. A tube is placed with the nose and to the stomach. The contents of the stomach are then suctioned out. Patients follow a clear liquid diet before gastrointestinal tract regains function. When patients go back to a normal diet, spicy and acidic foods ought to be avoided. It takes approximately 6 weeks to completely get over the surgery. The sutures that close patient skin can be taken off in 7 to ten days. Patients ought to maneuver around right after the operation to avoid the development of deep vein thrombus. Pain medicine, stool softeners, and antibiotics might be prescribed following an operation. Alternatives The most well-liked short-term treatment for gastric ulcers is drug therapy. A current review surveying medical articles published from 1977 to 1994 figured drugs for example cimetidine, ranitidine, famotidine, H2 blockers, and sucralfate were efficient, with omeprazole considered the "gold standard" for active gastric ulcer treatment. Surgical involvement, however, is suitable for individuals who don't react to medical therapy.
| 
 因缺血而行小肠分段切除及一期吻合术
因缺血而行小肠分段切除及一期吻合术
 肌肉活检 _ 如何进行肌肉活检
肌肉活检 _ 如何进行肌肉活检
 尿道下裂修复后包皮瘘和龟头隐裂
尿道下裂修复后包皮瘘和龟头隐裂
 通过外部方法对喉囊肿进行有袋化或去顶
通过外部方法对喉囊肿进行有袋化或去顶

 发表于 2013-2-2 17:20:24
发表于 2013-2-2 17:20:24
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡










