马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
Tracheotomy Tracheotomy Definition A tracheotomy is really a surgical treatment that reveals the windpipe. It's carried out in emergency circumstances, within the operating room, or at bedside of severely ill patients. The word tracheostomy may also be used interchangeably with tracheotomy. As it happens, however, tracheostomy generally refers back to the opening itself while a tracheotomy might be the actual operation. Who performs the process and where could it be done? Tracheotomy is conducted with a surgeon inside a hospital. Purpose A tracheotomy is conducted if sufficient air isn't dealing with the lungs, when the person cannot breathe without help, or perhaps is having issues with mucus along with other secretions engaging in the windpipe due to difficulty swallowing. Many reasons exist why air cannot arrive at the lungs. The windpipe might be blocked with a swelling; with a serious problem for the neck, nose, or mouth; with a large foreign object; by paralysis from the throat muscles; or with a tumor. The individual might be inside a coma, or require a ventilator to function air to the lungs for a long time. Questions patient should ask a doctor: - How will a patient look after his/her tracheotomy?
- How a lot of patient’s use noninvasive ventilation?
- Who is a right candidate for noninvasive ventilation?
Demographics Emergency tracheotomies are carried out when needed in a person needing one. Description Surgical tracheotomy The second kind of tracheotomy takes additional time and it is generally completed in an operating room. The doctor first constitutes a cut within the skin from the neck that lies within the trachea. This incision is incorporated in the lower the main neck between patient’s Adam's apple and the surface of the breastbone. The neck muscles are segregated and also the thyroid, which overlies the trachea, is generally reducing the center. The surgeon recognizes the rings of cartilage that define the trachea and cuts to the tough walls. Metallic or plastic tube, known as a tracheotomy tube, is introduced with the opening. This tube acts just like a windpipe and allows the individual to breathe. Oxygen or perhaps a mechanical ventilator might be connected towards the tube to create oxygen towards the lungs. A dressing is positioned round the opening. Tape or stitches are utilized to contain the tube in position. Following a nonemergency tracheotomy, the individual generally stays within the hospital for 3 to 5 days, unless there's a further complicating condition. It takes approximately fourteen days to recuperate fully in the surgery. Emergency tracheotomy There's two various procedures which are called tracheotomies. The foremost is done only in emergency circumstances and may be practiced very rapidly. The emergency room physician or doctor constitutes a cut inside a thin part of the voice box known as the cricothyroid membrane. A tube is introduced and attached to an oxygen bag. This emergency procedure may also be known as a cricothyroidotomy. Risks Long-term risks With time, other difficulties may develop carrying out a tracheotomy. The windpipe itself can become damaged for several reasons, which include pressure in the tube, infectious bacteria that form scarring, or friction from the tube that moves too much. Sometimes the opening doesn't close by itself following the tube is taken away. This risk is higher in tracheotomies with tubes residing in spot for 16 weeks or longer. In these instances, the wound is surgically closed. Increased secretions may exist in patients with tracheostomies, which need more frequent suctioning. Immediate risks There are many short-term risks related to tracheotomies. Serious bleeding is a possible problem. The voice box or esophagus might be damaged during surgery. Air can become trapped within the surrounding tissues or even the lung may collapse. The tracheotomy tube could be blocked by thrombus, mucus, or even the pressure from the airway walls. Obstruction could be prevented by suctioning, humidifying the environment, and selecting the right tracheotomy tube. Considerable infections are rare. High-risk groups The potential risks related to tracheotomies are higher within the following categories of patients: - smokers
- obese adults
- children, particularly newborns and infants
- alcoholics
- persons taking muscle relaxants , sleeping medicines, tranquilizers, or cortisone
- persons over 60
- persons with chronic diseases or respiratory infections
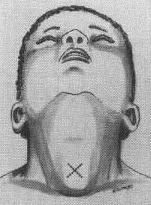
Diagnosis/Preparation Nonemergency tracheotomy Inside a nonemergency tracheotomy, there's time for that doctor to go over the surgery using the patient, to describe what's going to happen and why it's needed. The individual will be put under general anesthesia. The neck area and chest are then disinfected and surgical drapes are put within the area, establishing a sterile surgical field. Emergency tracheotomy Within the emergency tracheotomy, there isn't any time to explain the process or even the requirement for it towards the patient. The individual is positioned on his / her back with face upward (supine), having a rolled-up towel between patient’s shoulders. This positioning from the patient makes it much simpler for that doctor to feel and find out the structures within the throat. An area anesthetic is injected over the cricothyroid membrane. Normal results Normal results contain simple healing from the incision and successful upkeep of long-term tube placements. Morbidity and mortality rates The entire risk of death from the tracheotomy is under 5%. Aftercare Home care Following the patient is discharged; she or he will require help in patient’s own home to handle the tracheotomy tube. Warm compresses may be used to relieve pain in the incision site. The individual is suggested to maintain the region dry. It is suggested how the patient wear a loose scarf within the opening when going outside. She or he also needs to avoid connection with water, food particles, and powdery substances that may go into the opening and lead to serious difficulty in breathing. A doctor may prescribe pain medicine and antibiotics to reduce the chance of infections. When the tube will be saved in place permanently, the individual could be known a speech therapist to be able to learn how to consult with the tube in position. The tracheotomy tube might be changed four to ten days after surgery. Patients ought to start the majority of their normal activities after they leave a healthcare facility. Vigorous activity is bound for around 6 weeks. When the tracheotomy is permanent, additional surgery may be required to widen the opening, which narrows as time passes. Postoperative care A chest x-ray is usually taken, particularly in children, to check on if the tube is becoming displaced or if problems have taken place. A doctor may prescribe antibiotics to lessen the chance of infection. When the patient can breathe with no ventilator, the area is humidified; otherwise, when the tracheotomy tube would be to stay in place, the environment entering the tube from the ventilator is humidified. Throughout the hospital stay, the individual and or her members of the family will become familiar with how patient can look after the tracheotomy tube, which includes suctioning and clearing it. Secretions are taken out by passing an inferior tube to the tracheotomy tube. It requires most sufferers several days to sit in breathing with the tracheotomy tube. In the beginning, it will likely be hard even going to make sounds. When the tube enables some air to flee and pass within the vocal cords, then patients might be able to speak by holding a finger within the tube. Special tracheostomy tubes can also be found that assist in speech. The tube is going to be removed when the tracheotomy is temporary. Then patient’s wound will recover quickly in support of a little scar may remain. When the tracheotomy is permanent, the outlet stays open and, if it's no more needed, it will likely be surgically closed. Alternatives For many patients, there isn't any option to emergency tracheotomy. Some patients with pre-existing neuromuscular disease could be successfully handled with emergency noninvasive ventilation using a nose and mouth mask, instead of with tracheotomy. Patients who receive nonemergency tracheotomy when preparing for mechanical ventilation may get managed instead with noninvasive ventilation, with the right planning and education for the individual, caregiver, and medical staff. | 
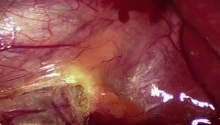
 腹腔镜胆囊切除术
腹腔镜胆囊切除术
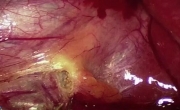
 坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
 改良根治性乳房切除术 - 第 2 部分分步讲解
改良根治性乳房切除术 - 第 2 部分分步讲解
 改良根治性乳房切除术 - 第 1 部分
改良根治性乳房切除术 - 第 1 部分

 发表于 2013-2-2 07:29:30
发表于 2013-2-2 07:29:30
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡