|
倒钩缝合术在腹腔镜胆囊切除术中胆管损伤修复中的应用——附2例报告

Fig. 1. Endoscopic retrograde cholangiography showed gallbladder stone (arrow),and common bile duct stones (arrow head). Anatomical variations of the biliary tractwere not evident.
图1.内镜逆行胰胆管造影显示胆囊结石(箭头),胆总管结石(箭头)。胆道有不明显的胆道解剖变异。
倒钩缝合术在腹腔镜胆囊切除术中胆管损伤修复中的应用——附2例报告

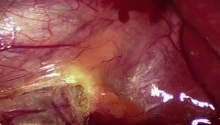
Fig. 2. Intraoperative findings: a) Bile spillage (arrow) was present in the gallbladderbed during gallbladder dissection, b) The injured small bile duct was evident (arrowhead). Repair using a titanium clip was unsuccessful.
图2.术中发现:一)胆汁溢出(箭头)在胆囊床在胆囊的解剖,b)受伤的小胆管明显(箭头)。使用钛夹修复是不成功的。
倒钩缝合术在腹腔镜胆囊切除术中胆管损伤修复中的应用——附2例报告

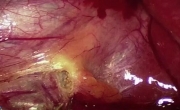
Fig. 3. Repair of bile duct injury: a) A running suture, using an absorbable 3-0 barbed suture (V-LocTM), was performed for the bile duct injury repair in the gallbladder bed,b) Bile spillage ceased after creating the running suture.
图3.胆管损伤的修复:a)连续缝合,用可吸收缝线3-0刺(v-loctm),为胆管损伤修复术中胆囊床,B)胆汁溢出后停止创造连续缝合。
倒钩缝合术在腹腔镜胆囊切除术中胆管损伤修复中的应用——附2例报告

Fig. 4. Bile spillage (arrow) was observed at the upper side of the gallbladder bed.
图4.胆汁溢出(箭头)在胆囊床上方观察。
倒钩缝合术在腹腔镜胆囊切除术中胆管损伤修复中的应用——附2例报告

Fig. 5. Following running suture using 3-0 V-LocTM, bile spillage ceased.
图5.以下以3-0 v-loctm连续缝合,胆汁溢出停止。 | 
 腹腔镜胆囊切除术
腹腔镜胆囊切除术
 坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
 改良根治性乳房切除术 - 第 2 部分分步讲解
改良根治性乳房切除术 - 第 2 部分分步讲解
 改良根治性乳房切除术 - 第 1 部分
改良根治性乳房切除术 - 第 1 部分

 发表于 2016-9-27 08:26:32
发表于 2016-9-27 08:26:32

 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主