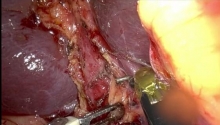
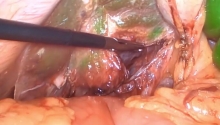
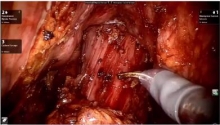
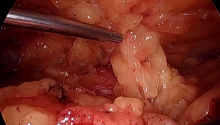
Subtotal colectomy for Large Bowel Obstruction from completely obstructing left colon carcinoma of the splenic flexure in a patient with previous subtotal gastrectomy and an antecolic Roux-en-Y gastroJJ reconstruction.
VIDEO #2
81 yrs old patient, previous appendectomy, hystero-oophorectomy, 9 years earlier gastric ca underwent subtotal gastrectomy (4/5) with an antecolic Roux-en-Y gastroJJ reconstruction. Spleen was preserved and is in situ.
Had adjuvant chemo. Otherwise well until now.
Presented to ED for Large Bowel Obstruction, vomiting, diffuse abdo pain and guarding and tenderness in RIF and right flank. Tachypnoeic. Meds: Warfarin
CT scan is presented, cecum dilated up to 12 cm, pneumatosis of the colonic wall of the cecum and right ascending colon.
Colonic stenting was considered an option but the Consultant Gastroenterologist considered it not feasible and contraindicated because too risky for the following reasons:
1) lesion too high up close to the splenic flexure in a patient with unprepared colon as seen from the CT
2) lesion seemed to be completely obstructing and possibility of failure consistent, given the difficult view
3) Patient with previous multiple laparotomies and an antecolic roux-en-Y and the risk of iatrogenic injuries was consistent due to limited mobility of the colon, fixed under the mesentery of the Roux en Y and the splenic flexure being stuck to the spleen in a patient with previous gastric surgery
4) Need of significant insufflation with subsequent high risk of perforation in a patient with pneumatosis of the right colon and suspected impending perforation and a cecum dilated up to 12 cm
Emergency Surgery for open laparotomy and subtotal colectomy with ileo-sigmoid hand-sewn anastomosis is started...
Operating Surgeon: Dr. Salomone Di Saverio MD, FACS, FRCS
Bologna, ITALY |

 骶骨阴道固定术 _ 穹窿脱垂 - 膀胱膨出
骶骨阴道固定术 _ 穹窿脱垂 - 膀胱膨出
 进行增强型手术 - 腹腔镜胆囊切除术用例
进行增强型手术 - 腹腔镜胆囊切除术用例
 肋下切口疝,Metin Ertem MD.FACS
肋下切口疝,Metin Ertem MD.FACS
 胆囊积脓_腹腔镜胆囊切除术治疗困难胆囊
胆囊积脓_腹腔镜胆囊切除术治疗困难胆囊

 发表于 2017-2-11 13:00:05
发表于 2017-2-11 13:00:05
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主