马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
本帖最后由 小针刀 于 2016-8-25 13:11 编辑
Choledochal cyst:Early experience by laparoscopic approach
胆总管囊肿早期腹腔镜手术的经验
Abstract
摘要
The management of choledochal cysts has evolved during the last 3 decades. Laparoscopic surgery has revolutionized the treatment of choledochal cyst (CC). We report our case, 2-year old female, in which total excision of cyst and Roux-en-Y hepaticoenterostomy is done by laparoscopic approach. In the hands of experts, laparoscopic excision of the CC is safe and effective approach. This is our first experience and our outcome has been good to a follow-up of 6 months. In our opinion, laparoscopic surgery is a safe treatment of choledochal cyst with less postoperative morbidity, a shorter length of stay and a lower blood loss when compared with open approach. Laparoscopic surgery may become the first choice procedure for choledochal cyst.
先天性胆总管囊肿的管理已经在过去的3年发生演变。腹腔镜手术已经彻底改变了胆总管囊肿的治疗(CC)。我们报告我们的案例,2岁的女性,其中囊肿全切除术和Roux-en-Y肝管肠吻合术是通过腹腔镜完成。在专家的手中,腹腔镜胆总管囊肿切除术是安全有效的方法。这是我们的第一次经验,我们的结果是好的在随访的6个月。据我们看来,腹腔镜手术是一种安全的治疗方法,与开放式比较腹腔镜胆总管囊肿术后并发症少、住院时间短、较低的失血量。腹腔镜手术可能成为胆总管囊肿的首选方法。
Key words
关键词
Choledochal cyst; Laparoscopic excision; Roux-en-Y hepaticojejunostomy
胆总管囊肿,腹腔镜切除术,肝总管空肠Roux-en-Y吻合术
Choledochal cyst (CC) is a fairly uncommon anomaly in which dilatations occur throughout the biliary tree. The management of choledochal cysts has evolved during the last 3 decades. Laparoscopic excision of choledochal cysts has increasingly gained acceptance and applicability since its first description by Farello [1], [2] and [3]. The potential advantages of laparoscopic cyst excision and Roux-en-Y hepaticojejunostomy (LH) include shorter recovery time, magnified view and improved cosmesis. Many reports confirm that laparoscopic approach is also feasibility and safe in children with long operative time and technique difficulties. Although the feasibility of laparoscopic resection of CC in early infancy is still unclear and needs further evaluation of the policy of surgical treatment timing in CC [3] and [4]. We report a case of 2-year-old girl with choledochal cyst (CC) of the common bile duct.
胆总管囊肿(CC)是一种相当罕见的异常现象,发生在胆道扩张。先天性胆总管囊肿的管理已经在过去的3年演变。腹腔镜胆总管囊肿切除术已经越来越得到认可和适用性,因为它的第一次描述由Farello[ 2 ]和[ 3 ]。腹腔镜囊肿切除术的潜在优势和Roux-en-Y肝管空肠吻合术(LH)包括较短的恢复时间,扩大术野并改善美观效果。许多报告证实,腹腔镜的方法是可行的和儿童安全的,但手术时间长、有技术难点。虽然腹腔镜胆总管囊肿切除术在婴儿早期的可行性,目前还不清楚,需要进一步评估政策、胆总管囊肿手术治疗的时机[ 3 ]和[ 4 ]。我们报告一个两岁的女孩胆总管囊肿病例(CC)在胆总管。
1. Case report
1、病例报告
A 2-year-old girl was admitted to our institute for repeated attack of pain over the right upper abdomen for last one month, anorexia and slight fever. The child was admitted and investigated. Laboratory studies showed only a slight increase in liver enzymes but bilirubin was in the range. On physical examination there was no hepato-splenomegaly, no abdominal mass but positive Murphy. Epigastric tenderness was a prominent feature. Abdominal ultrasound showed a dilatation of common byle duct (CBD) suggesting choledochal cyst (Fig. 1). Magnetic cholangio resonance confirmed the diagnosis (Fig. 2). According to the Todani classification we identified the CC as a type 1. The mini-invasive laparoscopic approach was done.
一个两岁的小女孩被送往我们的机构,持续一个月以上的右上腹部反复发作的疼痛,厌食和轻微的发烧。这个孩子被收治,并被调查。实验室研究表明,只有肝酶轻微的升高,但胆红素在范围内。体格检查无肝脾肿大,无腹部肿块但Murphy征阳性。上腹压痛是一个突出的特点。腹部超声显示扩张的胆总管(CBD)提示胆总管囊肿(图1)。磁共振确诊胆管(图2)。根据Todani的分类,我们发现CC作为类型1。该微创腹腔镜手术已完成。
Fig. 1. Abdominal ultrasound of choledochal cyst.

Fig. 1. Abdominal ultrasound of choledochal cyst.
图1.胆总管囊肿腹部超声。
Fig. 2. Magnetic cholangio resonance in choledochal cyst.

Fig. 2. Magnetic cholangio resonance in choledochal cyst.
图2.先天性胆总管囊肿胰胆管磁共振。
1.1. Surgical technique
1.1. 手术技巧
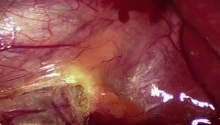
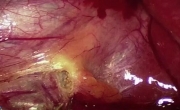
The patient was placed in the supine position. One trocar 12 mm for the camera through the umbilicus with open technique and four additional 5 mm ports were inserted: 2 were positioned at the right and left of the camera (below and above the umbilical line trasverse respectively), 1 under the xiphoid, and 1 in the right iliac fossa (Fig. 3). The peritoneum was inflated with CO2 gas maintaine a pressure of 8–10 mm Hg. On exploration, the CBD was found to be dilated with a maximum diameter of about 3 cm. After dissection, choledochotomy with colecystectomy was done. The jejunial gut is protruded through the umbilicus about 40 cm from Treitz and was cut and distally the jejunojejunostomy was performed extracorporeally at 80 cm from Treitz. After that the proximal end of the jejunal was passed retrocolic and hepaticojejunostomy Roux-en-Y was performed intracorporeally (Fig. 4). Subsequently it was put in the peritoneum and checked for torsion of the bowel. The mesenteric defect was closed and surgical drainage was inserted. No blood loss. The naso-gastric tube was removed in 2nd days, the drainage in 5th days and the length fasting was 7 days.
病人放置在仰卧位。一个套管针12毫米相机通过开放的技术和四个额外的5毫米端口脐部插入:2个被放置在相机的左右位置(分别低于和高于横向脐线),1个在剑突下,1个在右髂窝(图3)。腹膜后充气气体保持压力8–10毫米汞柱。探查中,胆总管被发现是扩张的最大直径约3厘米。解剖后,胆总管切开胆囊切除已完成。空肠的肠道通过脐中伸出约40厘米从Treitz韧带,被切断和在远端进行体外的空肠空肠造口约80厘米从Treitz韧带。之后,空肠近端通过结肠后与肝管空肠吻合术Roux-en-Y术通过生物体内(图4)。随后它被放在腹膜内,检查肠道扭转。肠系膜缺损闭合,并置入引流管。没有失血。鼻胃管在第2天拔除,第五天内引流及禁食时间为7天。
Fig. 3. Laparoscopic approach with trocars and surgeons’ arrangement.

Fig. 3. Laparoscopic approach with trocars and surgeons’ arrangement.
图3.腹腔镜手术与套管和外科医生的安排。
Fig. 4. Intraoperative choledochal cyst; Jejunojejunostomy; Retrocolic hepaticojejunostomy Roux-en-Y ...

Fig. 4. Intraoperative choledochal cyst; Jejunojejunostomy; Retrocolic hepaticojejunostomy Roux-en-Y.
图4.术中胆总管囊肿;空肠空肠吻合术;结肠后Roux-en-Y胆肠吻合术。
No early and late post-operative complication. Six months follow up are in the norm with no dilatation at ultrasonography, normal bilirubin and liver profile.
无早期和晚期术后并发症。术后随访六个月,超声无扩张、正常的胆红素和肝脏轮廓。
2. Discussion
2.讨论
The exact cause of choledochal cyst remains obscure. Many authors believe that they are congenital because most of cysts are diagnosed in infants and children. However, because approximately 20% are diagnosed in adults, including elderly patients, several theories have been postulated, as weakness of the wall of the bile duct; obstruction of the distal choledochus; combination of obstruction and weakness; reflux of pancreatic enzymes into the CBD secondary to an anomaly of the pancreaticobiliary junction. All of these theories are applicable to choledochal cyst type I, III and IV anomalies, but they cannot be used to explain type II and V in which the CBD is normal. Perhaps genetic factors play a role. Despite this, the two most accept theories are still reflux of pancreatic enzyme into the CBD secondary to an anomalous pancreatobiliary junction and obstruction of the distal CBD [3] and [5].
胆总管囊肿的确切病因仍不清楚。许多作者认为,他们是先天性的,因为大多数囊肿在婴儿和儿童被诊断。然而,因为大约20%的成人,包括老年患者被诊断,一些理论假设,例如胆管壁薄弱;胆总管远端梗阻;梗阻和薄弱相结合;胰腺酶进入CBD继发的胰胆管合流异常回流。所有这些理论都适用于胆总管囊肿I型,III和IV的异常,但它们不能用来解释II型和V型中的CBD是正常的。也许遗传因素扮演一个角色。尽管如此,两个最接受的理论仍然是胰液返流到CBD继发胰交界处异常和远端CBD [ 3 ]和[ 5 ]梗阻。
With the use of prenatal ultrasonography, an increasing number of choledochal cysts have been reported in the fetus. Incomplete gastric obstruction by a large cyst is one of the typical clinical manifestations in newborns and young infants [6]. The earliest reported choledochal cyst was detected in a fetus of 15 weeks', which may correspond to the timing of the formation of pancreatic enzyme.
随着产前超声检查的使用,越来越多的胆总管囊肿报道发现在胎儿。大囊肿不完全性胃梗阻是新生儿和婴幼儿的典型临床表现之一[ 6 ]。最早的报道在胎儿15周检测胆总管囊肿,这可能与胰腺酶形成的时间相对应。
Most centers prefer to excise the cyst shortly after birth, in the neonatal period, in fact surgical excision in this period has been shown to be technically feasible and well tolerated by patients [6], [7], [8], [9] and [10]. By the means of early surgery some authors perform either open or laparoscopic approach during neonatal period. It has been thought that neonatal surgery on a thin-walled choledochal cyst can be technically difficult and may lead to further anastomotic complications such as bile leakage or stricture [7], [11], [12] and [13]. Also for the mini-invasive surgery at neonatal period in literature, there are very few reviews in which some authors talk about this approach in fact most of patients have an age ranging from 12 months to 5 years and more. Neonatal laparoscopic surgery for CC is thought to be technically difficult and has potential risks, so they suggest that it is as safe as open surgery and has favorable outcomes after adequate experience have been achieved in laparoscopic CC excision [10].
大多数研究中心喜欢在出生后不久切除囊肿,在新生儿期,事实上,在这一时期的手术切除已被证明是在技术上是可行的,患者的耐受性良好[ 6 ],[ 8 ],[ 9 ]和[ 10 ]。通过早期手术的方式,一些作者在新生儿期进行开放或腹腔镜的方法。人们一直认为,新生儿外科对薄壁胆总管囊肿手术在技术上是困难的,可能会导致进一步的吻合口并发症如胆漏或狭窄[ 7 ]、[ 11 ]、[ 12 ]和[ 13 ]。在新生儿期的微创手术的文献中,也有很少的评论,一些作者谈论这种方法,事实上,大多数患者年龄从12个月至5岁不等。新生儿腹腔镜手术的外科手术被认为在技术上存在困难,有潜在的风险,所以他们建议,它是安全的开放手术,并有良好的预后,腹腔镜下胆总管囊肿切除术已经取得了足够的经验[ 10 ]。
Laparoscopic approach to CC was first described by Farelo et al. in a 6 years old child [14]. Since then, several authors highlighted the advantages of laparoscopic surgery in CC such as a magnified view, ease of identification and dissection of critical structures, particularly, in the main bile duct. They also emphasized the technical challenge of the hepaticojejunostomy as the most difficult and time-consuming step. The overall results of these data suggest that laparoscopic approach in the treatment of CC is feasible and safe with limited complications [10] and [11].
胆总管囊肿的腹腔镜手术是通过farelo等人首先描述。在一个6岁的孩子[ 14 ]。从那时起,一些作者强调了腹腔镜手术在胆总管囊肿的优点,如放大视图、易于识别和解剖关键结构,特别是在主胆管。他们还强调了胆肠吻合术的技术挑战是最困难和耗时的步骤。这些数据的整体结果表明,腹腔镜下的方法在治疗是可行的、安全的、有限的并发症[ 10 ]和[ 11 ]。
Also the technique of Roux-en-Y anastomosis under laparoscopy has been a matter of discussion. Although, some authors suggested using an EndoGIA but it is not feasible in children. Le et al. performed jejunojenunostomy intracorporeally and found that fully laparoscopic approach is exceedingly challenging and time-consuming.
同时腹腔镜下Roux-en-Y吻合术技术一直是一个讨论的问题。虽然,一些作者建议使用内镜缝合切割器(EndoGIA)但在儿童中是不可行的。Le等人,进行空肠空肠吻合术(jejunojenunostomy)发现完全腹腔镜手术是非常具有挑战性的和费时的。
We prefer the exteriorization of small bowel from the umbilical trocar incision commonly used to perform a jejunojenunostomy but intracorporeal hepaticojejunostomy Roux-en-Y anastomosis [10].
我们喜欢小肠外置常用进行脐孔切口进行空肠空肠吻合术(jejunojenunostomy),对接体内肝管空肠吻合Roux-en-Y吻合术[ 10 ]。
In contrast to the timing of surgery, currently with the technical advantages of minimally invasive surgery for pediatric CC the robotic surgical approach represents further progress. Probably the technical refinement and further miniaturization of robotic systems in the future would reduce the limiting effect of patient size in pediatric CC surgery [15] and [16].
与手术时机的对比,目前的微创手术的技术优势,为小儿胆总管囊肿机器人手术方式代表了进一步的进展。可能的技术细化和进一步小型化的机器人系统,将来会降低在小儿外科胆总管囊肿手术病人大小的限制作用[ 15 ]和[ 16 ]。
3. Conclusion
3.结论
Laparoscopic choledochal cyst excision is safe and feasible with many benefits of minimal access approach such as magnified view with more precise dissection and anastomosis, minimal tissue injury resulting in less blood loss, less post-operative pain, and adhesions with excellent cosmetic outcomes. Surgery should be performed early in order to prevent complications, in particularly malignancy and outcomes are better in pediatric patients. Long follow up is necessary to determine the advantages of laparoscopic approach in long term, especially in decreasing number of bowel adhesions. However, laparoscopic CC surgery requires great degree of technical skills and dexterity with experience in both biliary and advanced laparoscopic surgery to achieve excellent outcomes.
腹腔镜胆总管囊肿切除术是安全、可行的微创方法,如放大视图更精确的解剖和吻合的好处很多,最小的组织损伤导致出血量减少、术后疼痛轻、减少粘连并具有良好的美容效果。手术应早期进行,以防止并发症,特别是恶性肿瘤和儿科患者的效果是更好的。长期随访是必要的,以确定腹腔镜方法在长期的优势,尤其是在减少肠粘连的数量。然而,腹腔镜胆总管囊肿手术需要很大程度的技术技巧和熟练的胆道经验和先进的腹腔镜手术经验,以达到良好的效果。
References
[1]
S.L. Liu, L. Li, W.Y. Hou, J. Zhang, L.M. Huang, X. Li, et al.
Laparoscopic excision of choledochal cyst and Roux-en-Y hepaticojejunostomy in symptomatic neonates
J Pediatr Surg, 44 (2009), pp. 508–511
Article | PDF (257 K) | View Record in Scopus | Citing articles (16)
[2]
M. Diao, Long Li, W. Cheng
Role of laparoscopy in treatment of choledochal cysts in children
Pediatr Surg Int, 29 (2013), pp. 317–326
Full Text via CrossRef | View Record in Scopus | Citing articles (10)
[3]
G.A. Farello, A. Cerofolini, M. Rebonato, G. Bergamaschi, C. Ferrari, A. Chiappetta
Congenital choledochal cyst: video-guided laparoscopic treatment
Surg Laparosc Endosc, 5 (5) (1995 Oct), pp. 354–358
View Record in Scopus | Citing articles (98)
[4]
G.E. Besner
Pediatric choledochal cyst surgery: background, epidemiology, pathophysiology, surgery and pediatrics
(2015 Nov), pp. 1–7 emedicine
View Record in Scopus
[5]
K. Congo, M.F. Lopes, P.H. Oliviera, H. Matos, S. Basso, A. Reis
Outcomes of choledochal cysts with or without intrahepatic involvement in children after extrahepatic cyst excision and Roux-en-Y hepaticojejunostomy
Ann Hepatol, 11 (4) (2012), pp. 536–543
View Record in Scopus | Citing articles (12)
[6]
K.C. Soares, D.J. Arnaoutakis, I. Kamel, N. Rastegar, R. Anders, S. Maithel, et al.
Chledochal cysts: presentation, clinical differentiation and management
J Am Coll Surg, 219 (6) (2014 Dec), pp. 1167–1180
Article | PDF (1757 K) | View Record in Scopus | Citing articles (12)
[7]
H.L. Lugo-Vicente
Prenatally diagnosed choledochal cysts: observation or early surgery?
J Pediatr Surg, 30 (1995), pp. 1288–1290
Article | PDF (1633 K) | View Record in Scopus | Citing articles (44)
[8]
L. Li, S.L. Liu, W.Y. Hou, L. Cui, X.L. Liu, Z. Jun, et al.
Laparoscopic correction of biliary duct stenosis in choledochal cyst
J Pediatr Surg, 43 (2008), pp. 644–646
Article | PDF (158 K) | Full Text via CrossRef | View Record in Scopus | Citing articles (11)
[9]
C.G. Howell, J.M. Templeton, A.W. Flake, M. Glassman, J.M. Betts, C.L. Witzleben
Antenatal diagnosis and early surgery for choledochal cyst
J Pediatr Surg, 18 (4) (1983 Aug), pp. 387–393
Article | PDF (2445 K) | View Record in Scopus | Citing articles (70)
[10]
T.C. Mackenzie, L.J. Howell, A.W. Flake, N.S. Adzick
The management of prenatally diagnosed choledochal cysts
J Pediatr Surg, 36 (8) (2001 Aug), pp. 1241–1243
Article | PDF (50 K) | View Record in Scopus | Citing articles (51)
[11]
A. Cherqaoui, M. Haddad, C. Roman, G. Gorincour, J.Y. Marti, A. Bonnard, et al.
Management of choledochal cyst: evolution with antenatal diagnosis and laparoscopic approach
J Minim Access Surg, 8 (4) (2012 Oct), pp. 129–133
View Record in Scopus | Citing articles (7)
[12]
S. Suita, K. Shono, Y. Kinugasa, M. Kubota, S. Matsuo
Influence of age on the presentation and outcome of choledochal cyst
J Pediatr Surg, 34 (12) (1999 Dec), pp. 1765–1768
Article | PDF (4263 K) | View Record in Scopus | Citing articles (45)
[13]
L. Li, W. Feng, F. Jing-Bo, Y. Qi-Zhi, L. Gang, H. Liu-Ming, et al.
Laparoscopic assisted total cyst ecision of choledochal cyst and Roux-en-Y hepatoenterostomy
J Pediatr Surg, 39 (2004), pp. 1663–1666
Article | PDF (243 K) | View Record in Scopus | Citing articles (65)
[14]
J.H. Lee, S.H. Kim, H.Y. Kim, Y.H. Choi, S.E. Jung, K.W. Park
Early experience of laparoscopic choledochal cyst excision in children
J Korean Surg Soc, 85 (2013 Nov), pp. 225–229
Full Text via CrossRef | View Record in Scopus | Citing articles (3)
[15]
G.A. Farelo, A. Cerofolini, M. Rebonato, G. Bergamaschi, C. Ferrari, A. Chiappetta
Congenital choledochal cyst: video-guided laparoscopic treatment
Surg Laparosc Endosc, 5 (1995), pp. 354–358
[16]
N.Y. Kim, E.Y. Chang, Y.J. Hong, S. Park, H.Y. Kim, S.J. Bai, et al.
Retrospective Assessment of the validity of robotic surgery in comparison to open surgery for pediatric choledochal cyst
Yonsei Med J, 56 (3) (2015 May), pp. 737–743
Full Text via CrossRef | View Record in Scopus
原文:
 Choledochal cyst- Early experience by laparoscopic approach.pdf
(682.19 KB, 下载次数: 0, 售价: 99 香叶)
Choledochal cyst- Early experience by laparoscopic approach.pdf
(682.19 KB, 下载次数: 0, 售价: 99 香叶)
|
|

 腹腔镜胆囊切除术
腹腔镜胆囊切除术
 坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
 改良根治性乳房切除术 - 第 2 部分分步讲解
改良根治性乳房切除术 - 第 2 部分分步讲解
 改良根治性乳房切除术 - 第 1 部分
改良根治性乳房切除术 - 第 1 部分

 发表于 2016-8-25 08:10:27
发表于 2016-8-25 08:10:27
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡