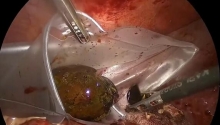
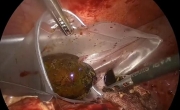
14. Graft implantation
1. Proximal aortic cuff
2. Opened aneurysm
3. Aortic graft
4. Running suture being performed, with medial to lateral insertion of the needle in the aorta
5. Biological glue
A polyester or polytetrafluoroethylen graft is chosen that is adapted to the diameter of the aortic neck and the type of bypass being done (aortic tube or bifurcated graft).
The body of the graft is cut to form a slightly oblique slant. Double-threaded 3.0 or 4.0 vascular suture, 1.2 m in length, is used.
The surgeon performs a conventional end-to-end anastomosis of the graft to the aorta while the first assistant maintains the suture under tension. The seal of this anastomosis is tested at the end of the procedure and biological glue is often added.
• Distal anastomoses
It is often necessary to reapply the self-retaining retractors to exert a slight downward traction on the wall. Calcifications and plaques may mandate modification of the distal anastomosis.
Two bulldog clamps were previously applied to the origin of the common iliac arteries. The distal part of the straight graft is cut with a slight slant to the desired length and a second, conventional anastomosis of the graft to the aorta is performed following the method described above.
Aorto-iliac bypass: when the aneurysm involves the bifurcation, distal anastomoses on the first few centimeters of the common iliac arteries are performed, above the previously applied bulldog clamps. The origin of each iliac artery is opened longitudinally and transversally. Each branch of the bifurcated graft is cut with a slant to the desired length.
A conventional end-to-end anastomosis on the graft to the common iliac artery is performed on each side, using 4.0 or 5.0 vascular suture.
Aorto-bifemoral bypass: involvement of the aneurysm down to the common iliac arteries requires an extension of the bypass to the common femoral arteries, or occasionally to the external iliac arteries.
In these cases, a classical approach via the right and left femoral triangles is used at the beginning of the procedure, before the abdominal approach. During this approach, and to avoid a secondary CO2 leak through the inguinal incisions, the arterial dissection below the crural arch must not be pursued.
During the abdominal approach, the common iliac arteries may be occluded with sutures or a linear stapler. Each branch of the graft must be placed in a subperitoneal anatomical position. A standard curved aortic clamp is introduced through the femoral triangle towards the aortic area. To guide the clamp during its insertion, the surgeon places his or her hand in the abdomen through the minilaparotomy.
Once each branch of the graft is exteriorized at the level of the femoral triangles, a conventional femoral-graft anastomosis is carried out with a 5.0 or 6.0 vascular suture. This anastomosis is done in an end-to-side fashion, permitting retrograde perfusion of the internal iliac arteries via the external iliac arteries.
Aorto-ilio-femoral bypass: if the aneurysm extends down asymmetrically, requiring a bypass onto one of the femoral axes, a limb of the graft is anastomosed to a common iliac artery. The other limb is passed into a retroperitoneal anatomical position and laterally anastomosed to the femoral bifurcation.
• Special cases
Bypass onto the iliac bifurcations: in the specific case where one or both internal iliac arteries must be perfused in an anterograde way (abdominal aortic aneurysm extending onto the origin of one or both internal iliac arteries) it is necessary to perform one or two anastomoses of the grafts to the iliac bifurcation(s).
On the left side, the laparoscopic dissection, which can be extended by an enlarged downward minilaparotomy, usually permits the surgeon to reach the iliac bifurcation and to perform the graft to iliac anastomosis at this level.
On the right side, laparoscopic dissection of the iliac bifurcation is difficult. A complementary 5 to 7 cm cutaneous incision (in the right flank) is usually preferable. The right iliac bifurcation can be reached by a retroperitoneal approach through this incision. The right limb of the graft can be easily placed in anatomical position.
• Case 2
Combined aorto-ilio-femoral occlusive lesions: the association of severe occlusive lesions with an abdominal aortic aneurysm is not frequent. It should be suspected in the presence of symptoms involving the legs (intermittent claudication, ischemic pain at rest or ischemic trophic disorders, disappearance of pulse). Systematic preoperative CT scan with contrast can often reveal occlusive lesions. In the presence of these signs, aorto-arteriography of the legs is mandatory.
In most cases, the type of bypass performed is an aorto-bifemoral restoration that takes this information into account.
1. Left inferior polar renal artery
2. IMA
Reimplantation of the IMA: the decision to reimplant the IMA into the left surface of the body of the graft or into the left branch of the bifurcated aortic graft can be made either before the procedure following the preoperative workup (occlusion of one or both internal iliac arteries) or if weak backflow is discovered when releasing the clamp from the IMA after opening the abdominal aortic aneurysm.
As in conventional surgery, an aortic patch is cut around the IMA ostium and reimplantation is performed through the minilaparotomy with a running 5.0 or 6.0 vascular suture. |

 急性胆囊炎——紧急救治策略
急性胆囊炎——紧急救治策略
 采用腹腔镜经筋膜腹外缝合术修复因 Morgagn
采用腹腔镜经筋膜腹外缝合术修复因 Morgagn
 腹腔镜全胃切除术治疗胃癌中采用线性吻合器
腹腔镜全胃切除术治疗胃癌中采用线性吻合器
 腹腔镜下Whipple手术治疗胰头肿瘤
腹腔镜下Whipple手术治疗胰头肿瘤

 楼主
楼主


 显身卡
显身卡