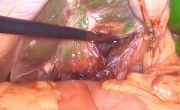
7. Dissection
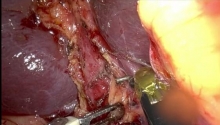
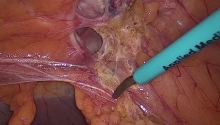
The procedure begins with the division of the supravesical peritoneum. The first assistant, on the patient’s right, pulls the prevesical peritoneum downwards with a grasper. For the incision of the peritoneum, we advise using monopolar laparoscopic scissors. The incision is made between the 2 umbilical arteries, above the bladder.
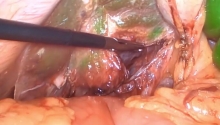
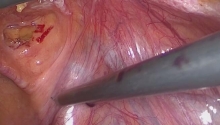
a. Dissection of the retropubic (Retzius’) space on the right
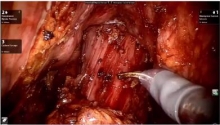
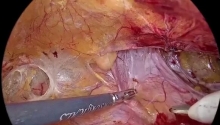
b. Dissection of the retropubic space on the left
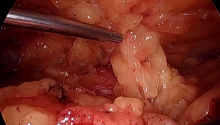
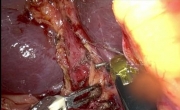
1. Pectineal (Cooper’s) ligament
2. Levator ani muscles
3. Insertion of the vagina on the levator ani muscles
4. Vagina
5. Vesical vein
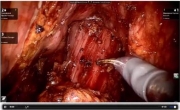
Once the supravesical peritoneum has been incised, the correct dissection plane, situated between the abdominal wall and the bladder, must be found. A common error is to dissect too close to the bladder, which can lead to a vesical injury. The dissection plane should be avascular.
Dissection of the retropubic space is pursued until the pectineal ligaments on the posterior surface of the superior pubic rami can be seen. These ligaments have a characteristic pearly white color. The dissection of the pectineal ligaments is progressively performed medially to laterally from the pubic symphysis. The external iliac vein should be visualized laterally. More caudad, the pelvic wall with the lateral insertion of the vagina on the tendinous arch of the levator ani muscles should be visible. The dissection is pursued laterally. The lateral edges of the bladder are retracted medially to visualize the most external part of the vaginal vault on each side. |

 复杂胆结石疾病的机器人治疗-3例视频描述
复杂胆结石疾病的机器人治疗-3例视频描述
 腹腔镜肝囊肿开窗术-使用 ICG 荧光
腹腔镜肝囊肿开窗术-使用 ICG 荧光
 ICG 荧光 - 3D CT 图像引导机器人结直肠手
ICG 荧光 - 3D CT 图像引导机器人结直肠手
 进行增强型手术 - 腹腔镜胆囊切除术用例
进行增强型手术 - 腹腔镜胆囊切除术用例

 发表于 2016-7-21 10:32:34
发表于 2016-7-21 10:32:34
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主