3. Therapy
General aims
There are 3 aims:
1. Re-expansion of the lung: can be achieved by chest tube drainage only, followed by suction therapy over several days with a negative pressure of about -20 cm H2O.
2. Leakage repair: usually requires surgery that includes suturing, stapling or gluing of the parenchymal leak.
3. Prevention of recurrence: involves different techniques whose goal is to obliterate the pleural space by creating adhesions between the visceral pleura and the chest wall. This pleurodesis may be performed surgically (abrasion, pleurectomy), thermally (cautery, laser) or pharmaceutically (instillation of antibiotics, talc, blood into the pleural space).
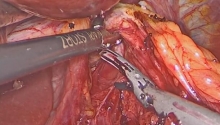
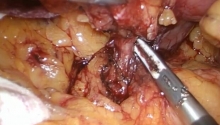
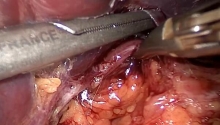
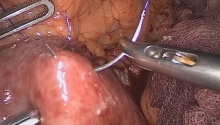
Conditions for VATS
Primary spontaneous pneumothorax: whether or not video-assisted thoracoscopic surgery (VATS) is indicated for a first occurrence of primary spontaneous pneumothorax is still under debate. The observed reduction of recurrences following VATS is in favor of the procedure. The cost (anesthesia, procedure, hospital stay) and the fact that a simple drainage cures 50% of the patients are detrimental to VATS.
After 10 years of experience with VATS, we believe that the technique is safe with a skilled thoracoscopic team (Hurtgen et al., 1996). Intrathoracic procedures can be performed as extensively and usually faster than via thoracotomy. Adhesions, eg along the phrenic nerve or along the subclavian vessels, may require conversion to thoracotomy.
Secondary pneumothorax: The same preconditions as for open thoracic surgery are required. VATS may be carried out by surgeons skilled in the technique. Those with less experience in VATS prefer thoracotomy for the treatment of secondary pneumothorax especially when emphysema is present and the lung tissue is fragile. In these patients, it is essential to treat the underlying obstructive pulmonary disease first. In all cases, conversion to thoracotomy can never be excluded. |

 腹腔镜下Whipple手术治疗胰头肿瘤
腹腔镜下Whipple手术治疗胰头肿瘤
 腹腔镜治疗正中弓状韧带综合征(MALS)——
腹腔镜治疗正中弓状韧带综合征(MALS)——
 腹腔镜治疗药物治疗失败后早期小肠梗阻复发
腹腔镜治疗药物治疗失败后早期小肠梗阻复发
 腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴
腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴

 发表于 2016-7-21 10:20:49
发表于 2016-7-21 10:20:49
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主