21. Reference
Balafrej S, Echarrab EM, el Ounani M, Mdaghri J, Amraoui M, el Alami FH et al. L'ulcère duodénal
hémorragique. Etude de la mortalité et des critères d'opérabilité. A propos de 557 cas.. J Chir
1997;134:406-9.
Gertsch P, Chow LW, Yuen ST, Chau KY, Lauder IJ. Long-term survival after gastrectomy for advanced
bleeding or perforated gastric carcinoma. Eur J Surg 1996;162:723-7.
Jordan PH, Jr., Thornby J. Twenty years after parietal cell vagotomy or selective vagotomy antrectomy for
treatment of duodenal ulcer. Final report. Ann Surg 1994;220:283-93; discussion 293-6.
Kyzer S, Binyamini Y, Melki Y, Ohana G, Koren R, Chaimoff C et al. Comparative study of the early
postoperative course and complications in patients undergoing Billroth I and Billroth II gastrectomy. World
J Surg 1997;21:763-6; discussion 767.
Lacaine F. Prise en charge de la maladie ulcéreuse gastrique en dehors de l'urgence: traitement
chirurgical. Gastroenterol Clin Biol 1996;20:S81-S83.
Lau WY, Leow CK. History of perforated duodenal and gastric ulcers. World J Surg 1997;21:890-6.
Michot F, Fraleu-Louer B. Prise en charge de la maladie ulcéreuse duodénale en dehors de l'urgence:
traitement chirurgical. Gastroenterol Clin Biol 1996;20:S64-S72.
Oka M, Maeda Y, Ueno T, Iizuka N, Abe T, Yamamoto K et al. A hemi-double stapling method to create
the Billroth-I anastomosis using a detachable device. J Am Coll Surg 1995;181:366-8.
Trias M, Targarona EM, Balague C, Bordas JM, Cirera I. Endoscopically-assisted laparoscopic partial
gastric resection for treatment of a large benign gastric adenoma. Surg Endosc 1996;10:344-6.
Witte CL. Is vagotomy and gastrectomy still justified for gastroduodenal ulcer? J Clin Gastroenterol
1995;20:2-3.
Witte CL. Gastric ulcer therapy. J Am Coll Surg 1997;184:337-8.
Yunfu L, Qinghua Z, Yongjia W. Pylorus and pyloric vagus preserving gastrectomy treating 125 cases of
peptic ulcer. Minerva Chir 1998;53:889-93. |

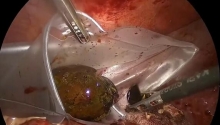
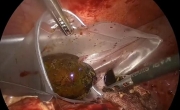 急性胆囊炎——紧急救治策略
急性胆囊炎——紧急救治策略
 采用腹腔镜经筋膜腹外缝合术修复因 Morgagn
采用腹腔镜经筋膜腹外缝合术修复因 Morgagn
 腹腔镜全胃切除术治疗胃癌中采用线性吻合器
腹腔镜全胃切除术治疗胃癌中采用线性吻合器
 腹腔镜下Whipple手术治疗胰头肿瘤
腹腔镜下Whipple手术治疗胰头肿瘤

 楼主
楼主 显身卡
显身卡