14. Reference
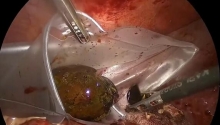
Peritonitis secondary to appendicitis is traditionally treated either by an enlarged McBurney’s incision to the flank and the right lower quadrant (in case of local peritonitis) or by a median incision (in case of general peritonitis). The laparoscopic approach makes it possible to avoid a large incision in the abdominal wall and almost eliminates the risk of wound infection.
For peritonitis, laparoscopy is an excellent approach with both diagnostic and therapeutic benefits.
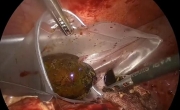
Laparoscopic exploration leads to an accurate diagnosis of the origin of the peritonitis in 85% of cases, and permits a precise assessment of the pathologies (perforated appendix, location of purulent collections).
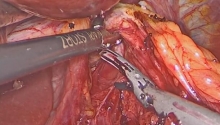
More than 80% of the cases of peritonitis from perforated appendices can be treated via laparoscopy. When conversion to laparotomy proves necessary, it is often possible to limit the size of the incision and to place it more accurately.
There are no complications specific to laparoscopy. However, caution must be exercised and certain technical rules must be observed.
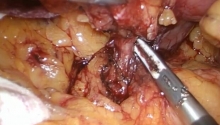
There are 2 risks related to the creation of a pneumoperitoneum in the context of intra-abdominal sepsis:
- hypercapnia: carbon dioxide absorption is increased by peritoneal inflammation,
- bacteremia: bacterial dissemination through the blood may occur either via bacterial translocation or direct bacterial passage through the lymphatics of the diaphragm and the thoracic duct. |

 急性胆囊炎——紧急救治策略
急性胆囊炎——紧急救治策略
 采用腹腔镜经筋膜腹外缝合术修复因 Morgagn
采用腹腔镜经筋膜腹外缝合术修复因 Morgagn
 腹腔镜全胃切除术治疗胃癌中采用线性吻合器
腹腔镜全胃切除术治疗胃癌中采用线性吻合器
 腹腔镜下Whipple手术治疗胰头肿瘤
腹腔镜下Whipple手术治疗胰头肿瘤

 楼主
楼主


 显身卡
显身卡