12. Dissection/lower rectum
• Introduction
Dissection of the lower rectum is difficult in obese patients or in patients with a narrow and deep pelvis. It is in contact with vascular and nerve structures that must be preserved (Enker et al., 2000; Heald et al., 1998). To preserve genitourinary functions, care must be taken to avoid the middle hemorrhoidal vessels (which are occasionally large) and the parasympathetic nerve branches originating from posterior sacral foramina.
Dissection is performed posteriorly, laterally, then anteriorly to the rectum, alternating the right and left side as the rectum is progressively freed.
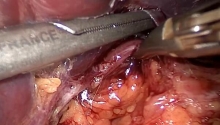
Laparoscopic freeing of the lower rectum is facilitated by the use of ultrasonic scissors or a vessel-sealing device.
The posterior dissection is continued caudally on the posterior side of the rectum, anterior to the sacrum, once the sacrorectal ligament (Waldeyer’s fascia) has been opened. Care must be taken to avoid the anterior sacral venous plexus running on the anterior surface of the periosteum of the sacrum. This plexus is formed from posterior branches that lead to large 2-5 mm foramina from the third to the fifth sacral vertebrae before draining into the venous plexus of the intrasacral canal.
Further down the rectum is supported by the rectococcygeal ligament. Sharp division of this structure, using ultrasonic scissors or after coagulation, helps gain 1 to 2 cm over the posterior surface of the rectum, and also assists identification of the anal sphincter.
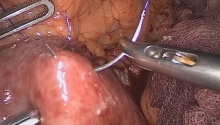
Dissection is facilitated by the posterior retraction of the rectum, and anterior retraction of the vagina or prostate with the use of an instrument introduced in the suprapubic trocar (trocar E), which grasps Denonvilliers’ fascia.
At this level, dissection of the anterior surface of the lower rectum can only be achieved after lateral rectal dissection (especially in men).
1. Prostate
2. Rectum
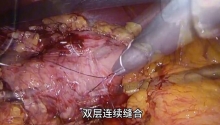
Low division of lateral ligaments exposes the lower pelvic space. This is done on the right side of the rectum, then on the left side. On the left side, the peritoneal reflection of the paracolic gutter should be incised down to the left lateral side of the rectum. One or more branches of the middle hemorrhoidal vessels joining the rectum on its anterior lateral surfaces are usually found on the lower part of lateral ligaments. These branches are infrequent, not always bilateral, and occasionally multiple. They should be controlled by clips or coagulation (bipolar forceps, vessel sealing device or ultrasonic scissors). At this level, the terminal branches of the pelvic nerve plexi run to the bladder, prostate, and genital organs (Enker et al., 1995; Enker et al., 2000). |

 女童尿道插管术
女童尿道插管术
 腹腔镜脾切除术治疗伴有EB病毒(EBV)感染
腹腔镜脾切除术治疗伴有EB病毒(EBV)感染
 大鹿角铸造肾结石肾镜取石术
大鹿角铸造肾结石肾镜取石术
 腹腔镜下右肾输尿管切除术伴膀胱袖口切除及
腹腔镜下右肾输尿管切除术伴膀胱袖口切除及

 楼主
楼主








 显身卡
显身卡