16. Reference
▶
Chapron C, Laforest L, Ansquer Y, Fauconnier A, Fernandez B, Breart G, Dubuisson JB.
Hysterectomy techniques used for benign pathologies: results of a French multicentre study. Hum Reprod 1999;14:2464-70.
Chapron C, Dubuisson JB. Total hysterectomy: laparoscopy or vaginal route? Arguments in favor of laparoscopy. Gynecol Obstet Fertil 2000;28:672-8.
Cosson M, Rajabally R, Querleu D, Crepin G. Hysterectomy: indications, surgical routes, cases for adnexal or cervical conservation. Eur J Obstet & Gynecol Reprod Biol 1998;80:5-15.
Johnson N, Barlow D, Lethaby A, Tavender E, Curr E, Garry R. Surgical approach to hysterectomy for
benign gynaecological disease. Cochrane Database Syst Rev 2005 CD003677. Update in: Cochrane
Database Syst Rev. 2006;(2):CD003677.
Lefebvre G, Allaire C, Jeffrey J, Vilos G, Arneja J, Birch C et al. SOGC clinical guidelines. Hysterectomy. J Obstet Gynaecol Can 2002;24:37-61.
Maresh MJ, Metcalfe MA, McPherson K, Overton C, Hall V, Hargreaves J et al. The VALUE national
hysterectomy study: description of the patients and their surgery. BJOG 2002;109:302-12.
Pokras R, Hufnagel VG. Hysterectomies in the United States, 1965-1984. Am J Public Health
1988;78:852-3.
Reich H. Laparoscopic hysterectomy. Surg Laparosc Endosc 1992;2:85-8.
Reich H, DeCaprio J, McGlynn F. Laparoscopic hysterectomy. J Gynecol Surg 1989;5:213-6.
Wattiez A, Canis M, Alexandre F, Pomel C, Bhoughizane S, Pouly JL et al. Uterine manipulator for laparoscopic hysterectomy. J Am Assoc Gynecol Laparosc 1995;4:S80.
Wattiez A, Canis M, Pouly L, Mage G, Bruhat MA. Technique coelioscopique de l’hystérectomie.
Journal de Coelio-chirurgie 1996;19:19-27.
Wattiez A, Cohen SB, Selvaggi L. Laparoscopic hysterectomy. Curr Opin Obstet Gynecol
2002;14:417-22.
Wattiez A, Soriano D, Cohen SB, Nervo P, Canis M, Botchorishvili R et al. The learning curve of total laparoscopic hysterectomy: comparative analysis of 1647 cases. J Am Assoc Gynecol Laparosc 2002;9:339-45.
Wattiez A, Soriano D, Fiaccavento A, Canis M, Botchorishvili R, Pouly J et al. Total laparoscopic hysterectomy for very enlarged uteri. J Am Assoc Gynecol Laparosc 2002;9:125-30. |

 腹腔镜下胆总管囊肿切除术及高级胆道重建术
腹腔镜下胆总管囊肿切除术及高级胆道重建术
 机器人辅助腹腔镜胆囊次全切除术和胆总管探
机器人辅助腹腔镜胆囊次全切除术和胆总管探
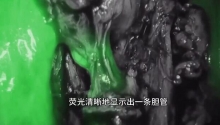
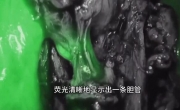 困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
 腹腔镜治疗85岁女性胆石性肠梗阻
腹腔镜治疗85岁女性胆石性肠梗阻

 楼主
楼主






 显身卡
显身卡