Inguinal hernia occurs more commonly in young boys as compared to girls and girls comprise less than 10% of all hernia cases. The most common symptoms of a girl with hernia would be an appearance of an inguinal swelling on and off when the child coughs, cries or is straining.
Whenever an inguinal hernia is suspected in a girl, it is important to be aware of a potential disorder of sex development. Upto 1-2% of all female children with hernia would be found to have Androgen insensitivity syndrome. In such a circumstance, a testis may be palpable in the inguinal region. In a girl with inguinal hernia, investigations should be done to rule out Androgen Insensitivity syndrome if there is any suspicion. Commonly, the contents of the hernia sac are omentum and/ or small bowel. In girls, ovaries have a propensity to herniate into the sac and undergo incarceration. If torsion sets in, this may lead to rapid infarction. Once diagnosed to have an ovary in the sac, surgery should be performed as early as possible to prevent such an eventuality. Sliding hernias are also known to occur in children where part of the bladder wall or fallopian tubes/ uterus have been found in the hernia defect.
Herniotomy for girls
Open Surgery for hernia in children called Herniotomy can be performed via a small inguinal or groin skin crease incision. We usually perform Herniotomy under inguinal block or caudal epidural analgesia along with sedation or under inhalational anesthesia with a laryngeal mask airway. Lower inguinal skin crease incision is marked centred over the pulsations of the femoral artery, over the expected internal ring. An incision is made through the deeper layers of skin until the fatty layer of the superficial fascia is encountered. In this plane there is a constant vein which needs to be coagulated as this vessel may be a source of minor bleeding if not recognised early on. Then membranous layer of the superficial fascia (Scarpa’s fascia) is divided with cutting diathermy and then the external oblique fascia is divided with a fine scissors along the length of the incision. The edges of the inferior leaf may be held with fine hemostats and everted; this maneuver opens up the inguinal canal.
When operating girls with inguinal hernia, it is important to open the sac and confirm the presence of round ligament and also make sure that none of the female internal organs such as fallopian tube, uterus, ovary are present in the sac. If the sac is empty, it is just ligated as usual. If there is a fallopian tube inside then it should be gently reposited back into the abdomen and sac ligated away from the tube.
In our experience, children who undergo open herniotomy for a unilateral hernia have a very rapid recovery, are discharged within a few hours and are running and playing shortly thereafter. Post-operative pain is not much of a concern as the cut is very small and no antibiotics are required. While for a laparoscopic hernia repair in child, three small cuts are needed, anesthesia is more and the advantage in terms of success is the same. Hence, a minimally invasive unilateral hernia repair by laparoscopic approach seems more invasive in terms of anesthesia and makes a purely extraperitoneal procedure an intraperitoneal one. We prefer to a do an open repair for a unilateral hernia is a child for these reasons and reserve laparoscopic approach for selected circumstances.
|

 腹腔镜全胃切除术治疗胃癌中采用线性吻合器
腹腔镜全胃切除术治疗胃癌中采用线性吻合器
 腹腔镜下Whipple手术治疗胰头肿瘤
腹腔镜下Whipple手术治疗胰头肿瘤
 腹腔镜治疗正中弓状韧带综合征(MALS)——
腹腔镜治疗正中弓状韧带综合征(MALS)——
 腹腔镜治疗药物治疗失败后早期小肠梗阻复发
腹腔镜治疗药物治疗失败后早期小肠梗阻复发

 发表于 2016-4-24 11:00:10
发表于 2016-4-24 11:00:10
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主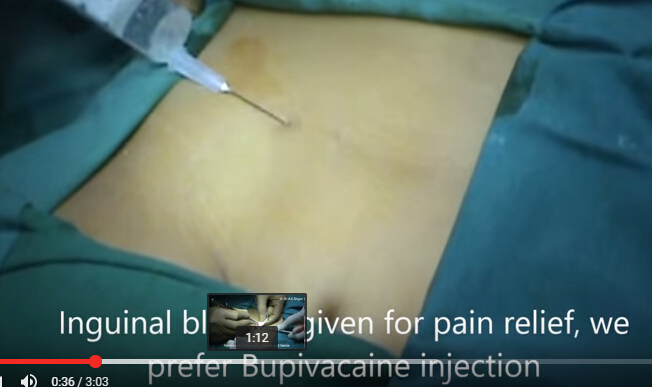
 发表于 2022-12-25 17:42:20
发表于 2022-12-25 17:42:20