Sex reassignment surgery for male-to-female involves reshaping the male genitals into a form with the appearance of, and, as far as possible, the function of female genitalia. Prior to any surgeries, patients usually undergo hormone replacement therapy (HRT), and, depending on the age at which HRT begins, facial hair removal. There are associated surgeries patients may elect to, including facial feminization surgery, breast augmentation, and various other procedures.
When changing anatomical sex from male to female, the testicles are removed, and the skin of foreskin and penis is usually inverted, as a flap preserving blood and nerve supplies (a technique pioneered by Sir Harold Gillies in 1951), to form a fully sensitive vagina (vaginoplasty). A clitoris fully supplied with nerve endings (innervated) can be formed from part of the glans of the penis. If the patient has been circumcised (removal of the foreskin), or if the surgeon's technique uses more skin in the formation of the labia minora, the pubic hair follicles are removed from some of the scrotal tissue, which is then incorporated by the surgeon within the vagina. Other scrotal tissue forms the labia majora.
In extreme cases of shortage of skin, or when a vaginoplasty has failed, a vaginal lining can be created from skin grafts from the thighs or hips, or a section of colon may be grafted in (colovaginoplasty). These linings may not provide the same sensate qualities as results from the penile inversion method, but the vaginal opening is identical, and the degree of sensation is approximately the same as that of most biological women, so pleasure should not be less.[citation needed]
Surgeon's requirements, procedures, and recommendations in the days before and after, and the months following, these procedures vary enormously.
Plastic surgery, since it involves skin, is never an exact procedure, and cosmetic refining to the outer vulva is sometimes required. Some surgeons prefer to do most of the crafting of the outer vulva as a second surgery, when other tissues, blood and nerve supplies have recovered from the first surgery. This relatively minor surgery, which is usually performed only under local anaesthetic, is called labiaplasty.
The aesthetic, sensational, and functional results of vaginoplasty vary greatly. Surgeons vary considerably in their techniques and skills, patients' skin varies in elasticity and healing ability (which is especially affected by smoking), any previous surgery in the area can impact results, and surgery can be complicated by problems such as infections, blood loss, or nerve damage.
Supporters of colovaginoplasty state that this method is better than use of skin grafts for the reason that colon is already mucosal, where as skin is not. However, many post-op trans women report that the skin used to line their vaginas develops mucosal qualities from months to years post-op. For others, lubrication is needed when having sex and occasional douching is advised so that bacteria does not start to grow and give off odors.
Because the human body treats the new vagina as a wound, any current technique of vaginoplasty requires some long-term maintenance of volume (vaginal dilation), by the patient, using medical graduated dilators, dildos, or suitable substitutes, to keep the vagina open. Sexual intercourse is not an adequate method of performing dilation. |

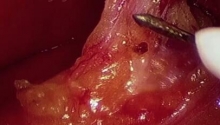
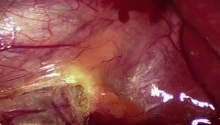
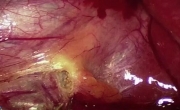
 腹腔镜胆囊切除术中胆囊动脉出血的处理
腹腔镜胆囊切除术中胆囊动脉出血的处理
 MAGPI 尿道下裂修复
MAGPI 尿道下裂修复
 腹腔镜胆囊切除术
腹腔镜胆囊切除术
 坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
坏疽性胆囊 - 腹腔镜胆囊切除术及技巧

 发表于 2016-4-6 11:00:06
发表于 2016-4-6 11:00:06
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主