Alfonso Rossetti, Ornella Sizzi, Massimo Mercuri
The main indications for a non-conservative treatment of endometriosis of the sigmoid-colon or rectum are the presence of a deep infiltration of the rectal or sigmoid wall wider then 3-4 cm or the presence of multiple infiltrations.
Another indication, luckily quite rare, is the stenosis of the rectal lumen.
The procedure starts with mobilization of sigmoid and descending colon until to reach the splenic flexure.
Then the descending colon is mobilized by blunt dissection from the Toldt fascia that is the anterior leaf of the Gerota (renal) fascia.
Afterwards the ureters are bilaterally dissected and the pararectal fossae (Okabayashy spaces) are bilaterally opened.
The thick adhesions between the rectum and the posterior wall of the uterus, the cervix and the vagina are dissected and all the endometriotic tissue adherent to uterus , cervix and vagina is removed.
The retrorectal space is opened dissecting the posterior wall of the rectum from the underlying connective tissue of the Toldt’s fascia that covers the sacrum and the piriformis muscle.
During this maneuver it is important to stay very close to the rectum to avoid damages to rectal nerves.
If the mobilization of the colon does not suffice, it is possible to cut the inferior mesenteric artery.
The rectum is mobilized dividing the lateral ligaments and the mesorectum up to the levator ani.
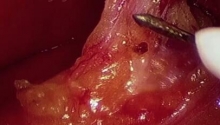
The rectum is divided distal to the lesion through a suprapubic minilaparotomy using a curved stapler.
The proximal colon is then brought down through the suprapubic minilaparotomic incision .
After that , the pathological portion of the rectum is asported, cutting the part with the deep infiltrating lesion.
A purse string is confectioned in the proximal bowel .
The bowel is then repositioned inside the abdominal cavity. Then a Lap Disc is applied to the minilaparotomic incision and the pneumoperitoneum is recreated.
The stapler is introduced through the anus and the spiked rod is introduced through a little cut in the bowel.
The anvil shaft is engaged to the stapling device and the stapling device is fired ,opened and withdrawn through the anus.
Then the arechecked the tissue donuts extracted .
Fibrin glue is applied on the suture and the integrity of the suture is checked .
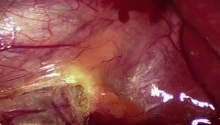
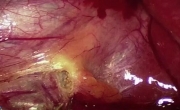
The last images show the multiple full thickness infiltrations of the rectum and the subsequent stenosis of the lumen. |

 腹腔镜胆囊切除术中胆囊动脉出血的处理
腹腔镜胆囊切除术中胆囊动脉出血的处理
 MAGPI 尿道下裂修复
MAGPI 尿道下裂修复
 腹腔镜胆囊切除术
腹腔镜胆囊切除术
 坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
坏疽性胆囊 - 腹腔镜胆囊切除术及技巧

 发表于 2016-1-10 11:00:01
发表于 2016-1-10 11:00:01
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主