- 快捷导航 |

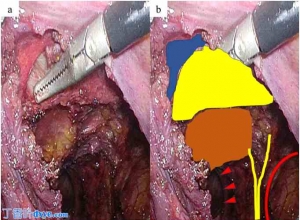
| 灵活的3D腹腔镜辅助复位和经皮固定治疗髋臼骨折-新手术方案的介绍 Flexible 3D laparoscopic assisted reduction and percutaneous fixation of acetabular fractures- Introduction to a new surgical option Abstract The gold standard for fractures of the acetabulum is to perform an open reduction and internal fixation in order to achieve anatomical reduction. In a well-defined subset of patients, percutaneous techniques may be employed but achieving reduction by closed means can be challenging especially for fractures with large degrees of displacement. Such patient may include elderly patients who may not have the physiologic reserve to withstand open approaches. In our paper, we present a new option using laparoscopic assisted reduction of the acetabular fracture and percutaneous fixation. The young obese patient refused all forms of blood products transfusion and presented with a displaced transverse posterior wall fracture. While we do not recommend routine use of such technique and recognize its numerous limitations, we present it as an alternative strategy in a small subset of patients. 摘要 髋臼骨折的金标准是进行切开复位内固定,以达到解剖复位的目的。在一个明确的子集的患者,经皮技术可以采用,但通过封闭的方式实现减少可能是具有挑战性的,特别是对于大程度的位移骨折。这种病人可能包括老年患者谁可能没有生理储备能够承受开放的方法。在我们的论文中,我们提出了一个新的选项,使用腹腔镜辅助减少髋臼骨折和经皮固定。年轻的肥胖病人拒绝所有形式的血液制品输血,并提出了一个流离失所的横向后壁骨折。虽然我们不建议常规使用这种技术,并认识到它的众多的局限性,我们提出它作为一种替代策略,在一个小的子集的患者。 KEYWORDS: Fractures of the acetabulum; Laparoscopic assisted acetabular fracture reduction; Laparoscopic retroperitoneal 3D dissection; Percutaneous acetabular fracture fixation 关键词: 髋臼骨折;腹腔镜辅助髋臼骨折复位术;腹腔镜腹膜后三维解剖;经皮髋臼骨折内固定术 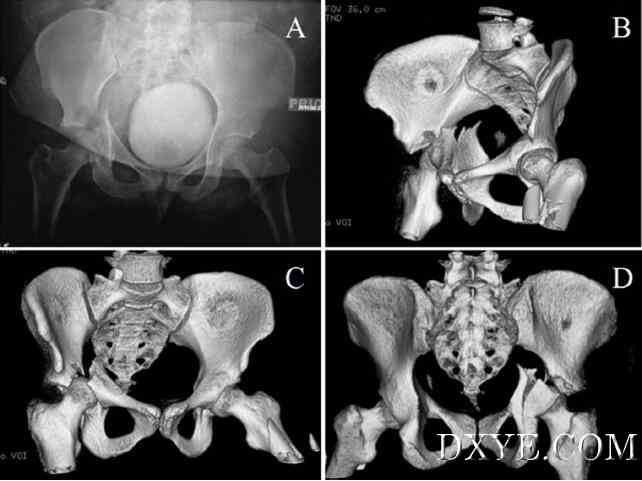 Fig. 1. Pelvic radiograph AP view (A) of the right transverse posterior wall acetabular fracture and 3D CT reconstructions of the right acetabular fracture (B–D). 图. 1. 骨盆正位X线片(A)AP视图的右横髋臼后壁骨折、右髋臼骨折的CT三维重建(B–D)。  Fig. 2. In A, the distal femoral traction bow is connected to a ceiling pulley system through a sterile rope attached to a 5-gallon bucket, which can be filled with saline/sand bags. In B and C images the patient’s pelvis has been bolted to the flat top table using external fixation connected to sterile Thompson table attachments. In Fig. 2D, a Schanz pin has been placed in the femoral neck and attached laterally in order to obtain a lateral vector of traction. 图. 2. 在A中,股骨远端牵引弓通过连接到一个5加仑桶中的无菌绳索,其可填充有生理盐水/砂袋连接到天花板的滑轮系统。在B和C的图像的病人的骨盆已经用螺栓固定到使用连接到无菌汤普森表附件外固定平顶表。在图如图2D所示,一个Schanz针已经被放置在股骨颈和侧向连接以获得牵引力的横向向量。 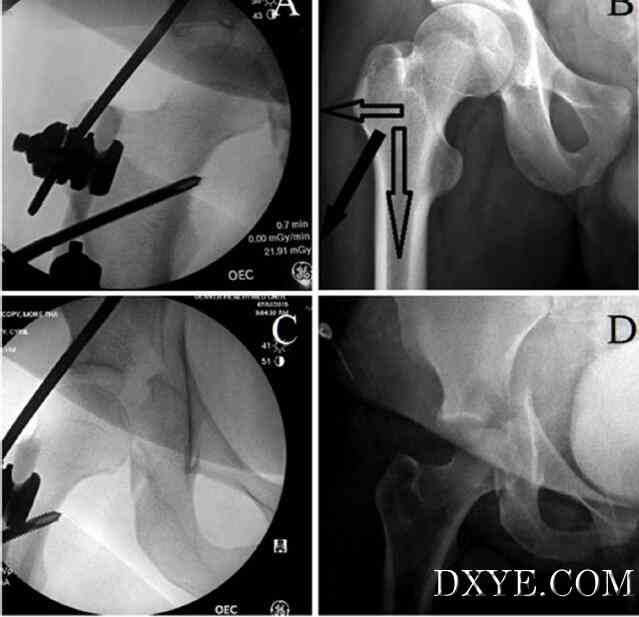 Fig. 3. In A, fluoroscopy AP image of the right hip showing the lateral Schanz pin in the femoral neck and in B the vectors of pull. In C a fluoroscopic AP image of the right hip showing the reduction of the protrused femoral head under the sourcil thanks to the traction system. In D, AP radiograph of the right hip showing the initial degree of displacement and protrusion of the femoral head. 图. 3. 在A中,右髋部的透视AP图像示出了股骨颈和B中拉力的矢量的横向Schanz针。在C右髋的一个荧光的AP图像表示protrused股骨头的sourcil由于牵引系统下的减少。在D中,右髋部的AP X射线照片表示位移和股骨头突起的初始程度。 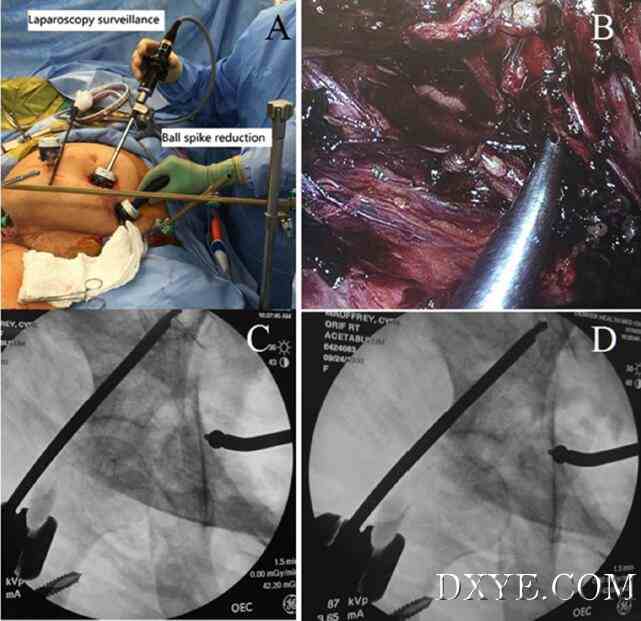 Fig. 4. In A, intra operative clinical photograph of the laparoscopy portion of the case. In B, intraoperative laparoscopic view of the right quadrilateral plate with a ball spike pusher positioned on the quadrilateral plate just below the obturator nerve. In C and D, fluoroscopic view of the right acetabular fracture reduced by the ball spike pusher. 图. 4. 在A一个手术中的腹腔镜部分的临床照片。B,一个球穗推位于四边形板下方的闭孔神经的腹腔镜术中视野对四边形板。在C和D,透视右侧髋臼骨折的球穗推缩小视图。 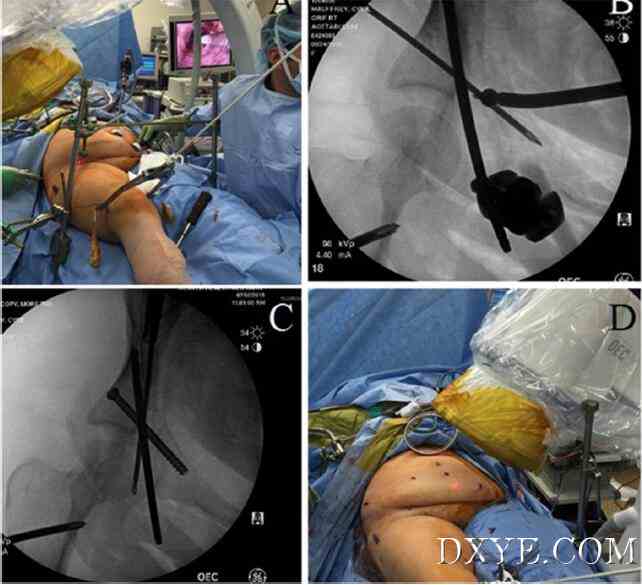 Fig. 5. In A, intraoperative picture of the laparoscopic portion of the procedure with the ball spike in place through one of the laparoscopic portals. In B, fluoroscopic AP view of the right acetabulum showing the placement of an antegrade anterior column guidewire. In C, AP fluoroscopic view of the right acetabulum during antegrade insertion of a posterior column guidewire. In D, postoperative clinical photograph of the surgical incisions. 图. 5. 在A,用到位球秒杀过程中,通过腹腔镜的门户网站之一的部分腹腔镜术中的图片。在B中,右髋臼荧光AP视图表示顺行前柱导丝的位置。在C中,后柱导丝顺行插入时AP右髋臼的透视图。在D中,手术切口的术后临床照片。 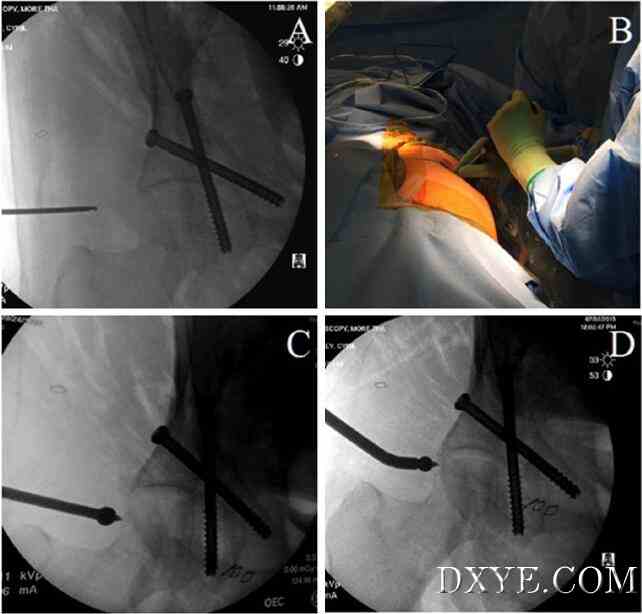 Fig. 6. In A, identification of the displaced posterior wall fragment using a right obturator oblique view. In B, clinical picture of the prone patient showing the ball spike in place through a small posterior incision. In C, fluoroscopic obturator oblique view of the right acetabulum showing the ball spike placed over the displaced posterior wall fragment and the reduced wall fragment in D. 图. 6. 在A,使用右闭孔斜位的移位的后壁骨折鉴定。在B,多发性病人的临床表现,通过一个小的后切口的球钉的位置。在C,透视闭孔的右髋臼显示球穗放在移位的后壁骨折斜视角和D.减少壁片段右髋臼透视闭孔斜位视图 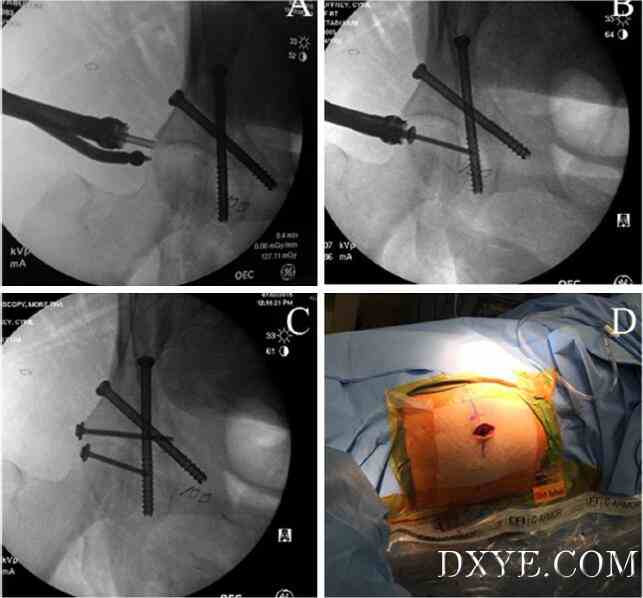 Fig. 7. In A–C, fluoroscopic views of an obturator oblique view of the right acetabulum during percutaneous fixation of the posterior wall fragment. In D, clinical photograph of the prone patient with surgical incision for percutaneous fixation of the posterior wall fragment. 图. 7. 在A-C,后壁骨折经皮固定在右侧髋臼闭孔斜位透视视图。在D,易发患者手术切口经皮内固定治疗后壁骨折的临床分析。 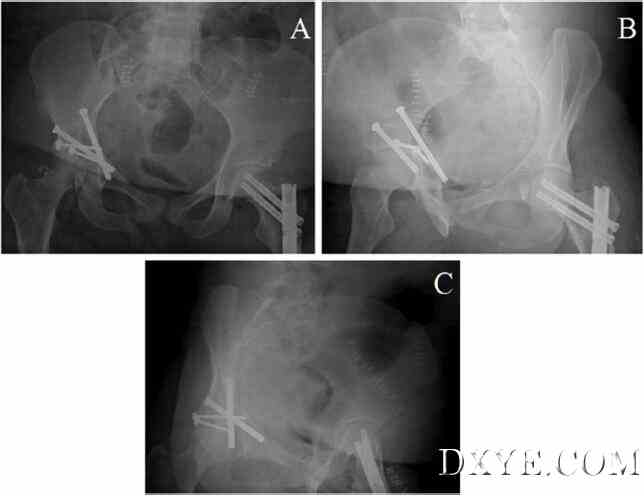 Fig. 8. Postoperative AP (A), iliac oblique (B) and obturator oblique (C) radiographs of the pelvis. 图. 8. 术后AP(A),髂骨斜(B)和闭孔斜位(C)骨盆X光片。 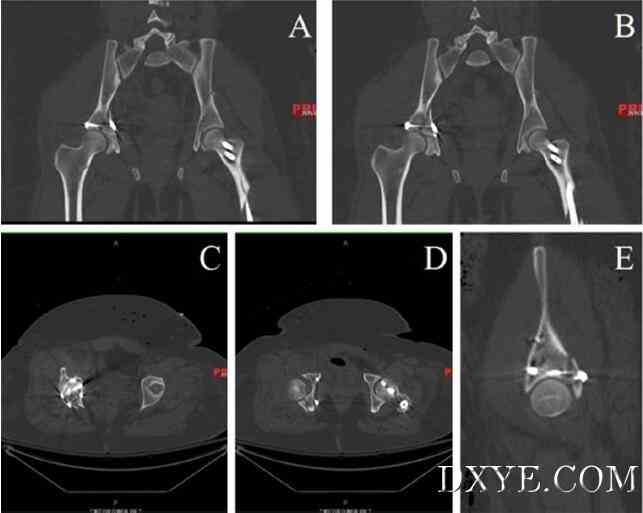 Fig. 9. Postoperative CT scan obtained at day 1 postop. Coronal (A and B), Axial (C and D) and sagittal (E) views. A 1.5 mm articular step off is seen in image D. 图. 9. 在后第1天的运算获得术后CT扫描。冠状(A和B),轴向(C和D)和矢状(E)的意见。1.5毫米关节的退出被认为是在图像D. 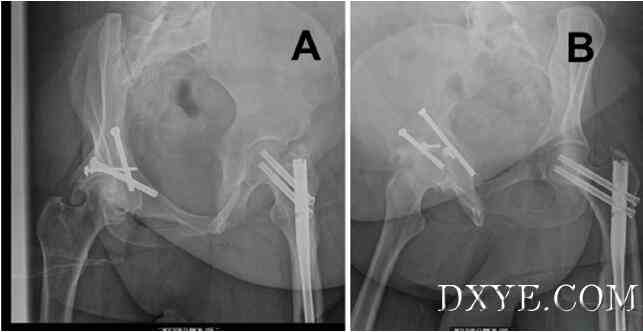 Fig. 10. Obturator oblique (A) and Iliac oblique (B) radiographs of right pelvis at 1 year post fixation showing some heterotopic ossification. 图. 10. 闭孔斜位(A)和髂骨斜(B),1年后固定骨盆右侧显示一些异位骨化的X光片。 全文:http://www.dxye.com/thread-24316-1-1.html |