- 快捷导航 |

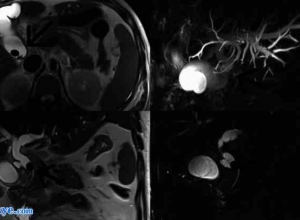
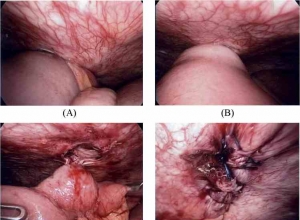
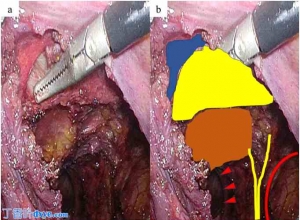
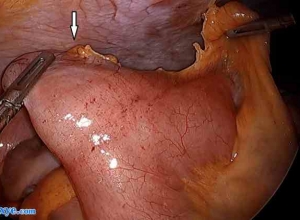
| 倒钩缝合术在腹腔镜胆囊切除术中胆管损伤修复中的应用——附2例报告 Effectiveness of a barbed suture in the repair of bile duct injury during laparoscopic cholecystectomy- Report of two cases Abstract 摘要 INTRODUCTION: 简介: Bile duct injury during laparoscopic cholecystectomy occurs in rare cases. We report two cases using barbed suture for repair in bile duct injury during laparoscopic cholecystectomies. 腹腔镜胆囊切除术中胆管损伤的罕见病例。我们报告两例采用倒钩缝合在腹腔镜胆囊切除术中胆管损伤的修复。 PRESENTATION OF CASES: 病例报告: The first patient was a 73-year-old woman who underwent elective laparoscopic cholecystectomy for cholecystolithiasis. When the gallbladder was dissected from the bed, bile spillage was observed and an injured small bile duct was detected. The bile duct could not be managed using a titanium clip. The second patient was an 83-year-old woman who underwent emergent laparoscopic cholecystectomy for gallbladder torsion. After the gallbladder was dissected from the bed, bile spillage was observed. In both cases, a running suture, of absorbable monofilament 3-0 barbed suture, was used to laparoscopically repair the injuries. 第一个病人是一个73岁的女人,择期行腹腔镜胆囊切除术治疗胆囊结石。在胆囊的解剖床上,胆汁溢出观察一只受伤的小胆管的检测。胆管不能使用钛夹管理。第二例患者是一位83岁的女性,接受急诊腹腔镜胆囊切除术治疗胆囊扭转。在胆囊的解剖床上,观察胆汁溢出。在这两种情况下,连续缝合,可吸收线缝合3:0刺,用于腹腔镜手术修复损伤。 DISCUSSION: 讨论: Laparoscopic repair of a bile duct injury is technically challenging, especially in the gallbladder bed where suturing is very difficult because of the tangential approach and the risk of additional liver laceration. Barbed sutures have the benefit of being knotless, thus, performing a running suture is not difficult, even in laparoscopic procedures. Further, absorbable and monofilament threads are generally better suited for biliary surgery, compared with non-absorbable and braided sutures, because of the potential association of the other types of materials with bile duct stone and stricture formation. 一个胆管损伤腹腔镜修补术是技术上的挑战,尤其是在胆囊床上,缝合很困难因为切线的方法和额外的肝裂伤的风险。带刺的缝合线的好处是没有结的,因此,执行运行缝合并不困难,甚至在腹腔镜手术。此外,可吸收单丝线通常更适合胆道手术,相对于非吸收性和编织缝合,因为潜在关联的其他材料的类型与胆管结石及狭窄的形成。 CONCLUSION: 结论: We believe that the V-Loc™ device is an effective and appropriate option for bile duct injuries that occur during laparoscopic cholecystectomies, particularly around the gallbladder bed, and it is especially useful for surgeons unfamiliar with intracorporeal knot tying. 我们相信,v-loc™装置是有效的和适当的胆管损伤腹腔镜胆囊切除术中发生的选择,尤其是在胆囊床,它是特别有用的外科医生熟悉体内打结。 原文:http://www.dxye.com/thread-24294-1-1.html 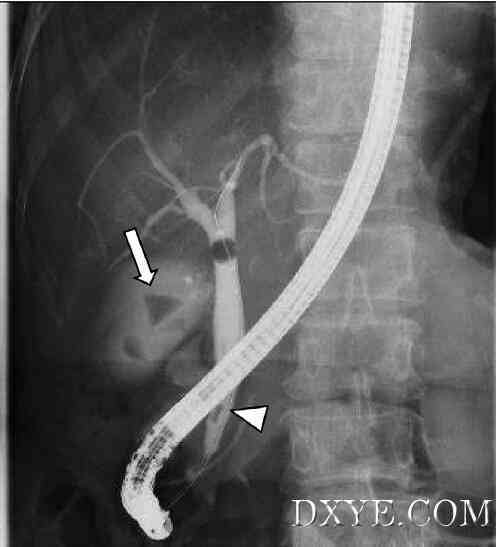 Fig. 1. Endoscopic retrograde cholangiography showed gallbladder stone (arrow),and common bile duct stones (arrow head). Anatomical variations of the biliary tractwere not evident. 图1.内镜逆行胰胆管造影显示胆囊结石(箭头),胆总管结石(箭头)。胆道有不明显的胆道解剖变异。 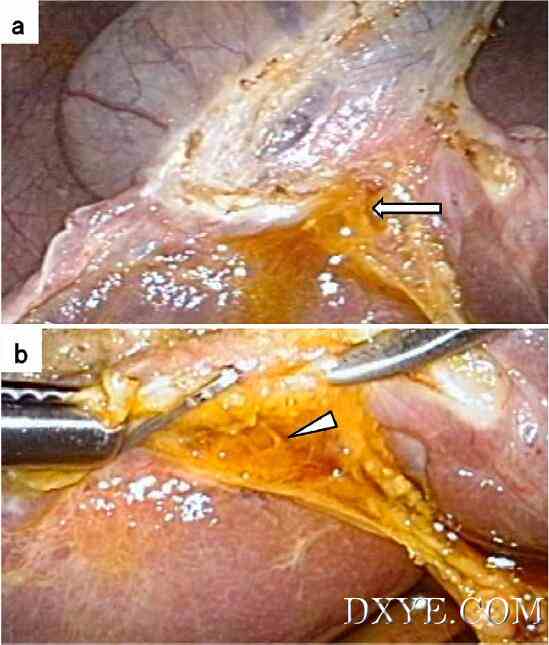 Fig. 2. Intraoperative findings: a) Bile spillage (arrow) was present in the gallbladderbed during gallbladder dissection, b) The injured small bile duct was evident (arrowhead). Repair using a titanium clip was unsuccessful. 图2.术中发现:一)胆汁溢出(箭头)在胆囊床在胆囊的解剖,b)受伤的小胆管明显(箭头)。使用钛夹修复是不成功的。 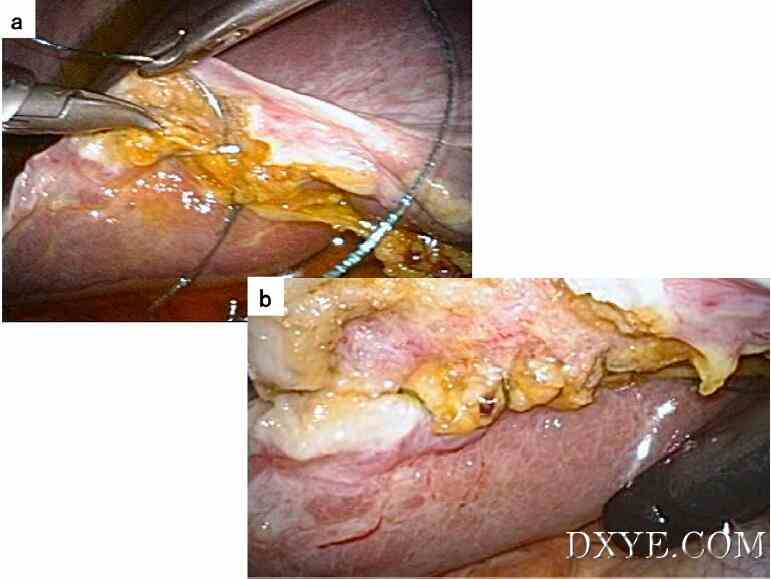 Fig. 3. Repair of bile duct injury: a) A running suture, using an absorbable 3-0 barbed suture (V-LocTM), was performed for the bile duct injury repair in the gallbladder bed,b) Bile spillage ceased after creating the running suture. 图3.胆管损伤的修复:a)连续缝合,用可吸收缝线3-0刺(v-loctm),为胆管损伤修复术中胆囊床,B)胆汁溢出后停止创造连续缝合。 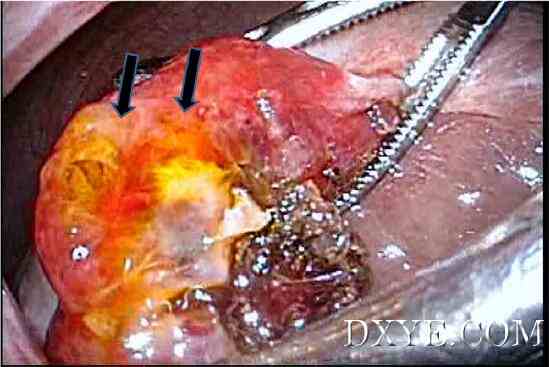 Fig. 4. Bile spillage (arrow) was observed at the upper side of the gallbladder bed. 图4.胆汁溢出(箭头)在胆囊床上方观察。  Fig. 5. Following running suture using 3-0 V-LocTM, bile spillage ceased. 图5.以下以3-0 v-loctm连续缝合,胆汁溢出停止。 |