19. Reference
▶
1. Overby DW, Apelgren K, Richardson W, Fanelli R, Society of American Gastrointestinal and Endoscopic Surgeons. SAGES guidelines for the clinical application of laparoscopic biliary tract surgery. Surg Endosc 2010;24:2368-86.
2. Berci G, Hunter J, Morgenstern L, Arregui M, Brunt M, Carroll B, Edye M, Fermelia D, Ferzli G, Greene F, Petelin J, Phillips E, Ponsky J, Sax H, Schwaitzberg S, Soper N, Swanstrom L, Traverso W. Laparoscopic cholecystectomy: first, do no harm; second, take care of bile duct stones. Surg Endosc 2013;27:1051-4.
3. Strasberg SM, Brunt LM. Rationale and use of the critical view of safety in laparoscopic cholecystectomy. J Am Coll Surg 2010;211:132-8.
4. Eikermann M, Siegel R, Broeders I, Dziri C, Fingerhut A, Gutt C, Jaschinski T, Nassar A, Paganini AM, Pieper D, Targarona E, Schrewe M, Shamiyeh A, Strik M, Neugebauer EA, European Association for Endoscopic Surgery. Prevention and treatment of bile duct injuries during laparoscopic cholecystectomy: the clinical practice guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc 2012;26:3003-39.
5. Laurence JM, Tran PD, Richardson AJ, Pleass HC, Lam VW. Laparoscopic or open cholecystectomy in cirrhosis: a systematic review of outcomes and meta-analysis of randomized trials. HPB 2012;14:153-61.
6. Sun S, Yang K, Gao M, He X, Tian J, Ma B. Three-port versus four-port laparoscopic cholecystectomy: meta-analysis of randomized clinical trials. World J Surg 2009;33:1904-8.
7. Gurusamy KS, Vaughan J, Ramamoorthy R, Fusai G, Davidson BR. Miniports versus standard ports for laparoscopic cholecystectomy. Cochrane Database Syst Rev 2013;8:CD006804.
8. Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA 2003;289:1639-44.
9. Sajid MS, Leaver C, Haider Z, Worthington T, Karanjia N, Singh KK. Routine on-table cholangiography during cholecystectomy: a systematic review. Ann R Coll Surg Engl 2012;94:375-80.
10. Alvarez FA, de Santibañes M, Palavecino M, Sánchez Clariá R, Mazza O, Arbues G, de Santibañes E, Pekolj J. Impact of routine intraoperative cholangiography during laparoscopic cholecystectomy on bile duct injury. Br J Surg 2014;101:677-84.
11. Sheffield KM, Han Y, Kuo YF, Townsend CM Jr., Goodwin JS, Riall TS. Variation in the use of intraoperative cholangiography during cholecystectomy. J Am Coll Surg 2012;214:668-79.
12. Gurusamy KS, Bong JJ, Fusai G, Davidson BR. Methods of cystic duct occlusion during laparoscopic cholecystectomy. Cochrane Database Syst Rev 2010;10:CD006807.
13. Gurusamy KS, Samraj K, Mullerat P, Davidson BR. Routine abdominal drainage for uncomplicated laparoscopic cholecystectomy. Cochrane Database Syst Rev 2007;4:CD006004.
14. Picchio M, Lucarelli P, Di Filippo A, De Angelis F, Stipa F, Spaziani E. Meta-analysis of drainage versus no drainage after laparoscopic cholecystectomy. JSLS 2014;18:00242.
15. Kahokehr A, Sammour T, Soop M, Hill AG. Intraperitoneal use of local anesthetic in laparoscopic cholecystectomy: systematic review and metaanalysis of randomized controlled trials. J Hepatobiliary Pancreat Sci 2010;17:637-56.
16. Sheffield KM, Riall TS, Han Y, Kuo YF, Townsend CM Jr, Goodwin JS. Association between cholecystectomy with vs without intraoperative cholangiography and risk of common duct injury. JAMA 2013;310:812-20. |

 儿童单端口,机器人,经膀胱膀胱阴道瘘修复
儿童单端口,机器人,经膀胱膀胱阴道瘘修复
 腹腔镜 Whipple 手术(切除期)
腹腔镜 Whipple 手术(切除期)
 机器人为脑死亡但有心跳的尸体捐献者进行自
机器人为脑死亡但有心跳的尸体捐献者进行自
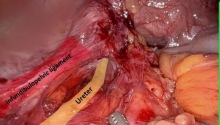
 机器人输尿管重建不可吸收夹侵蚀输尿管
机器人输尿管重建不可吸收夹侵蚀输尿管

 发表于 2015-3-17 19:22:22
发表于 2015-3-17 19:22:22

 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 发表于 2016-2-27 04:09:06
发表于 2016-2-27 04:09:06
 楼主
楼主