6. Trocar placement
• Pneumoperitoneum
The pneumoperitoneum is generally performed with a Veress needle in the umbilical region with the insufflation of CO2 up to a pressure of 10 mm Hg to 12 mm Hg, with an initial inflow of 1L/min. With scoliosis, previous operations on the upper abdominal quadrants and in infants, an open procedure is suggested. We have no experience in cholecystectomy with patients younger than 1 year, for whom an open technique is always indicated because of the high risk of a blind puncture of the abdomen.
If an open technique is required, the incision is performed under direct visualization of the fascia and peritoneum and a stay suture is positioned on the fascia to fix a 5 mm or 10 mm reusable trocar.
Four trocars are used. Apart from the optical trocar, the position of the other trocars is not constant because the size of the abdominal wall varies with the age of the patients.
A: 5-10 mm (10 mm for patients older than one year), in the umbilical region
B: 5 mm, in the right side along the median axillary line or the midclavicular line below the navel
C: 5 mm, in the right subcostal region along the mammary or epigastric line
D: 5-10 mm, in the left subcostal region along the median clavicular line |

 腹腔镜下胆总管囊肿切除术及高级胆道重建术
腹腔镜下胆总管囊肿切除术及高级胆道重建术
 机器人辅助腹腔镜胆囊次全切除术和胆总管探
机器人辅助腹腔镜胆囊次全切除术和胆总管探
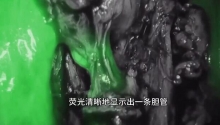
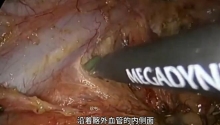
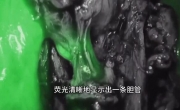 困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
 腹腔镜治疗85岁女性胆石性肠梗阻
腹腔镜治疗85岁女性胆石性肠梗阻

 发表于 2016-7-21 09:56:22
发表于 2016-7-21 09:56:22
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主