1. Introduction
▶
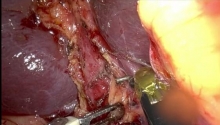
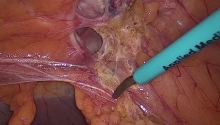
Laparoscopic colon resection for malignancy is performed in advanced laparoscopic centers in order to have the patient benefit of the advantages of a minimally invasive procedure (smaller wounds, shorter hospital stay and earlier food intake). However, because an open right colectomy is a straightforward and simple procedure in comparison to the laparoscopic approach which demands more time, resources and equipment, many are questioning whether or not the laparoscopic approach offers any added benefits.
This chapter describes techniques for laparoscopic right colon resection for cancer. Although early studies report a high port-site recurrence rate, the most important randomized controlled multicenter studies such as Barcelona, COST, COLOR, CLASICC trials (Bonjer et al., 2007) appear to refute this risk and demonstrate that the oncological outcomes are at least equivalent. Additionally, the “Lacy” trial demonstrated improved cancer-related survival for stage III disease in the laparoscopic group (Lacy et al., 2008).
While the data for long-term survival still needs to be confirmed, the multiple short-term benefits of laparoscopy have been confirmed by many studies: these are smaller wounds, less postoperative pain, shorter hospital stay and earlier oral food intake.
The method used in this laparoscopic right colectomy will be analysed and discussed, thus allowing for a constructive comparison of the varying techniques utilized by other experts.
This chapter will describe the technique that was used for this intervention so that it may be reproduced, but it is important to note that the approach can vary according to each case. |

 经皮肾镜取石术 (PCNL) 治疗大肾结石 - 现
经皮肾镜取石术 (PCNL) 治疗大肾结石 - 现
 包皮环切术
包皮环切术
 骶骨阴道固定术 _ 穹窿脱垂 - 膀胱膨出
骶骨阴道固定术 _ 穹窿脱垂 - 膀胱膨出
 进行增强型手术 - 腹腔镜胆囊切除术用例
进行增强型手术 - 腹腔镜胆囊切除术用例

 发表于 2016-7-21 09:16:24
发表于 2016-7-21 09:16:24
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主