3. Classification
• Hiatal hernias

1. Thoracic esophagus
2. Thoracic cavity
3. Right crus
4. Left crus
5. Abdominal esophagus
6. Fundus of the stomach
Hiatal hernias cause most gastroesophageal reflux diseases (GERD).
• Type I hiatal hernias
• Classification

Type I, or sliding hiatal hernias, have an intact attenuated phrenoesophageal ligament.
They can be subclassified according to 3 anatomically distinct stages of evolution.
• Stage 1

Sliding hiatal hernias occur when the abdominal esophagus migrates through the hiatus while the gastroesophageal junction (GEJ) and stomach remain below.
As the abdominal esophagus migrates, the EGV disappears due to the widening of the esophagogastric angle, and the LESE diminishes due to the loss of anatomical relationships and extrinsic pressures.
This may not be appreciated on endoscopy or barium study.
This would explain the reports of GERD without a hiatal hernia.
• Stage 2

Stage 2 sliding hiatal hernias occur when the gastroesophageal junction and stomach migrate above the diaphragm.
The EGV can reform above the diaphragm, preventing reflux.
This may explain reports of sliding hiatal hernias without GERD.
• Stage 3

Stage 3 sliding hiatal hernias have a shortened esophagus with fixation of the gastroesophageal junction above the diaphragm due to scarring.
True stage 3 hiatal hernias are rare.
• Type II hiatal hernias

Type II, or paraesophageal hiatal hernias, occur through a defect in the phrenoesophageal ligament.
The gastroesophageal junction nonetheless remains in the abdominal cavity. |

 腹腔镜下胆总管囊肿切除术及高级胆道重建术
腹腔镜下胆总管囊肿切除术及高级胆道重建术
 机器人辅助腹腔镜胆囊次全切除术和胆总管探
机器人辅助腹腔镜胆囊次全切除术和胆总管探
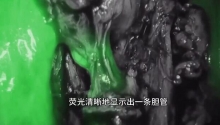
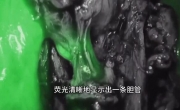 困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
 腹腔镜治疗85岁女性胆石性肠梗阻
腹腔镜治疗85岁女性胆石性肠梗阻

 发表于 2016-7-21 08:22:35
发表于 2016-7-21 08:22:35
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主